Burning mouth syndrome (BMS) is challenging to diagnose, especially in its primary form, and its prevalence is difficult to establish, due to the absence of clear diagnostic criteria. BMS affects women more frequently and has a notable prevalence, varying across studies between 0.7% and 15% in the general population. The average age of patients is around 60 years old. The increased prevalence of BMS in women is associated with menopause, with the majority of female patients presenting symptoms around this period. Psychological factors such as stress, anxiety and depression are regarded as triggering or exacerbating factors for BMS symptoms. Sleep disorders are commonly encountered in patients with burning mouth syndrome and can contribute to the symptomatology of this condition. The clinical profile of BMS patient involves female predominance, a connection with menopause, and an association with psychological factors such as stress and sleep disorders. Specific symptoms, frequent referrals to various specialists, and associations with general conditions complicate the diagnosis and management of this condition.
An overview of the clinical profile of patients with burning mouth syndrome
rezentarea profilurilor clinice ale pacienţilor cu algie bucală nespecifică
First published: 28 septembrie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ORL.60.3.2023.8583
Abstract
Rezumat
Algia bucală nespecifică (ABN) este dificil de diagnosticat, în special în forma sa primară, iar prevalenţa este dificil de stabilit, din cauza absenţei criteriilor clare de diagnostic. ABN afectează mai frecvent femeile şi are o prevalenţă ridicată, variind, în funcţie de studii, între 0,7% şi 15% în populaţia generală. Vârsta medie a pacienţilor este de 60 de ani. Prevalenţa crescută a ABN la femei este asociată cu menopauza, iar majoritatea pacientelor prezintă simptome în jurul acestei perioade. Factorii psihologici, cum ar fi stresul, anxietatea şi depresia, sunt consideraţi factori declanşatori sau amplificatori pentru simptomele ABN. Tulburările de somn sunt frecvent întâlnite la pacienţii cu ABN şi pot contribui la simptomatologia acestei afecţiuni. Profilul clinic al pacientului cu algie bucală nespecifică implică predominanţa la femei, legătura cu menopauza şi asocierea cu factori psihologici precum stresul şi tulburările de somn. Simptomele specifice, adresabilitatea frecventă către diferiţi specialişti şi asocierile cu afecţiuni generale complică diagnosticul şi gestionarea acestei afecţiuni.
Introduction
Definition. Burning mouth syndrome (BMS) is a complex condition characterized by a sensation of generalized or localized burning or pain within the oral cavity, occurring daily for more than two hours per day, for over three months, without any evident alteration in the oral mucosa and/or laboratory findings(1).
Classification. BMS was initially classified as a distinct condition by the International Headache Society in 2004. Etiologically, BMS can be classified into two forms(2):
1. Primary form (essential/idiopathic), in which local/systemic organic causes cannot be identified, but which involves pathogenic neurological pathways ranging from peripheral to central regions. The characteristics of this primary form can be summarized in the following definition: “an idiopathic pathological state characterized by a burning sensation in the oral mucosa, which appears clinically healthy”(3).
2. Secondary form, determined by local, systemic or psychological factors.
For this reason, BMS is a challenging condition to diagnose, especially in its primary form, despite many years of clinical research and experimental studies(4).
Prevalence. Establishing the true prevalence of BMS is challenging due to the lack of rigorous diagnostic criteria, as there are no clear distinguishing criteria between the primary and secondary forms of BMS(5). Regardless of the specific clinical presentation, this condition exhibits a notable prevalence which varies in studies ranging from 0.7% to 14.8-15%(6,7). Sardella et al. (2013) documented a BMS prevalence in the general population ranging from 0.5% to 5%, while Tammiala-Salonen et al., in 1993 (mentioned by Gurvits and Tan, 2013), reported a rate of 15% in the Finnish adult population(8-10). The varying incidence in different studies can largely be attributed to the lack of well-defined criteria for diagnosing the two forms of BMS(7,10).
The importance of the study derives primarily from the impact of the symptoms on the patient’s quality of life. The degree of manifestation and influence on the quality of life by BMS is variable, ranging from allowing the patient to carry out normal activities to severely compromising their life. The first category of patients tend to detach from the syndrome’s symptomatology, not reporting it, compared to another category that includes patients who are “obsessed”, even expressing thoughts of suicide. The distinct behavior exhibited by patients is determined not only by the psychological perception of the sensation, but also by the fluctuating intensity of the BMS symptoms throughout the day and over an extended period of time. Consequently, severe cases identified during the anamnesis exhibit a constant distribution of symptom intensity throughout the day, compelling the patients to obsessively focus on their well-being(3).
Discussion
General predisposing factors (average age of patients/sex/menopause). Burning mouth syndrome has a clear predisposition determined by age and sex. According to the study conducted by Gurvits and Tan (2013), BMS can affect patients in any age group, ranging from 27 to 87 years old; however, the average age of disease onset is 61 years old(10).
Women are affected 2.5 to 7 times more frequently than men. In various studies, the gender ratio of affected patients (female/male) varied from 3/1 to 16/1(5). Up to 90% of female patients with BMS are around the menopausal period, and the onset interval of BMS symptoms ranges from three years before to 12 years after menopause(10).
In a study that examined the relationship between sociodemographic characteristics and clinical features of patients with BMS, conducted from September 2011 to March 2012 at the University of Naples, on a sample of 75 patients, the mean age of the sample was 61.17 years old (±11.75), and the female-to-male ratio was 3/1, confirming that the prevalence of BMS is higher in females, especially in those around the age of 60(5).
In another study conducted on a sample of 65 patients evaluated at the Dental School of Aichi-Gakuin University in Nagoya, Japan, it was observed that the mean age of participants was 60 ± 9.9 years old, with a gender ratio of 5.5 women to 1 man. The results highlighted that BMS-type disorders have a significantly higher prevalence among middle-aged and older women(11).
Another research carried out on a cohort of 91 patients examined at the Dental Clinic of the University of Barcelona from 2000 to 2011 revealed that the mean age of patients was 69.9 years old (with an age range from 40 to 85 years old), and the female-to-male ratio was 14/1(6).
According to Klasser and Epstein (2012), BMS is rarely observed in patients under the age of 30, and its prevalence can increase from 3 to 12 times with advancing age(12). This aspect is also mentioned by Adamo et al. in a study from 2015(5).
In the analysis conducted by Gao et al. (2009) on the factors involved in the etiology of BMS in a group of 87 BMS cases, 66 (75.9%) were women, of whom 47 (54%) were in the climacteric or post-climacteric period. According to the conclusions of this study, in women with BMS in the menopausal period, serum hormonal dosages showed significantly higher concentrations of FSH and significantly lower levels of estradiol(13).
Additionally, Grushka (2014) asserts that this decrease in estrogen concentration during the menopausal period is responsible for accentuating the sensory alterations perceived in the context of BMS(3,14).
Sociodemographic characteristics of patients. In an investigation conducted by Adamo and colleagues in 2015, analyzing the correlation between the sociodemographic characteristics and the clinical features of patients diagnosed with BMS, it was found that the prevalence of this type of disorder was more significant among female patients (74.7%), married patients (76%), those without a professional occupation (80%), and in those with a medium level of education(5).
These findings may pave the way for further research to analyze in detail the interactions between these variables and the clinical aspects of BMS.
The onset of painful symptomatology is generally spontaneous, seemingly unrelated to any precipitating factor. However, some patients associate the onset of the disease with a series of events, such as previous dental procedures, medication treatments or stressful life events. In the case of a study conducted by Adamo et al., the most commonly reported event correlated with the onset of the condition was the presence of stressful life events (34 patients; 45%)(5).
According to the study carried out by Klasser et al. in 2011, it was observed that 43% of the patients in the study group reported the triggering event of the disease as unknown. In the same context, 27% of patients stated that the onset of the burning sensation was associated with dental treatment, 16% linked the onset to the administration of a new medication, and 14% indicated other medical or personal events. Notably, it is mentioned that none specifically reported stress factors as potential triggers of the condition(15).
The time period from the onset of the condition to the initial presentation at medical consultation varies according to studies in the specialized literature. Thus, in a study conducted in 2009 by Gao et al., the duration of this mentioned period ranged from 10 days to 10 years, with an average value of nine months(13).
In a study conducted by Spanemberg et al. in 2015, on a sample of 78 patients treated at the São Lucas Hospital in Brazil, it was highlighted that one-third of the patients with BMS had a duration of this interval ranging from one to three years(16).
The degree of seeking consultations with various specialists prior to the initial diagnosis of BMS. López et al. (2013), following a study that evaluated responses to different treatments and clinical outcomes in patients with oral pain, concluded that a significant proportion of cases undergo repeated consultations with various medical specialties without benefiting from substantial solutions or improvements concerning their health issue. In this research undertaken on patients who were consulted at the Oral Medicine Unit of the Dental Clinic at the University of Barcelona between 2000 and 2011, the results indicated that, out of a total of 91 patients, 74 consulted different specialists, including dermatologists (30%), otolaryngologists (10%), psychiatrists (3%), psychologists (2%), neurologists (2%), homeopaths (1%), and rheumatologists (0.5%). Among these 74 patients, 45 (approximately 49.45%) consulted a specialist, 13 patients (approximately 14.25%) were seen by up to four specialists, and 16 of these patients visited other dental practitioners(17).
Characteristics of oral symptomatology. In the specialized literature, the sensation of burning within the oral mucosa represents the main symptom of BMS, and the level of pain can range from mild to severe(5). Data from this study indicate that the sensation of oral burning was present in 59 patients (79%) and for most patients, the intensity was moderate, assessed on the pain scale at approximately 5-8 cm.
Burning symptoms within the oral mucosa can affect one or more distinct regions. According to the specialized literature, the tip and dorsal surface of the tongue, as well as the lips, are the most commonly affected areas(16). Additionally, it is noted that the pain often appears localized in multiple sites.
Thus, the results of a prevalence-focused study performed on 62 women diagnosed with BMS indicate that 88.7% of cases present symptom localization at the anterior two-third of the tongue(18). In a study conducted by Spanemberg et al. in 2012, on a sample of 58 BMS patients treated at the Oral Medicine Division of the São Lucas Hospital, Pontifical Catholic University of Rio Grande do Sul (Brazil), it was found that the areas most predisposed to subjective symptom manifestations were the tongue (78.3%), lips (25.8%) and hard palate (31%)(19).
Associated manifestations
Xerostomia is a commonly associated symptom in patients with primary BMS, with a prevalence ranging between 34% and 39%. Grushka et al. (2003) even identified a higher prevalence, reaching at least 60% in the cases studied(20).
In a study regarding prevalence and associated factors conducted on 62 women diagnosed with BMS, Baharvand et al. (2014) found that 37.8% of them presented xerostomia as an associated symptom, indicating that more than one-third of BMS patients experienced xerostomia(18).
A higher frequency of this symptom (60%) was identified in a study conducted by Adamo et al. (2015), making it the most commonly associated symptom(5). Additionally, the same percentage (61%) was highlighted by Klasser et al. (2011) in a group of 49 patients(15).
Dysgeusia. Other specialized studies report higher percentages of patients presenting with dysgeusia – 48.3%(19).
Moreover, other research reflects more substantial proportions of patients experiencing dysgeusia. According to Baharvand et al. in 2014, it was observed that 48.3% of patients exhibited this associated symptom(18).
In the context of dysgeusia within BMS, other relevant studies have supported this observation. The interpretation of this association, according to Grushka’s hypothesis (2014), involves the damage to the gustatory fibers of the VII and/or IX nerves, which induces the loss of inhibition and an increase in the sensory-excitatory hyperexcitability of these cranial nerves(3,14).
Sleep disturbances. A specialized study conducted by Gao et al. in 2009, on a group of 87 patients, aiming to assess and analyze risk factors involved in the onset of BMS, reported more substantial percentages of patients experiencing sleep difficulties (56.3%)(13).
Chainani-Wu et al. (2011), in a study focused on evaluating whether sleep disorders predispose to BMS, demonstrated that these patients reported a higher degree of sleep difficulties compared to the control group. The study suggests that sleep disturbances could be a risk factor associated with the development of BMS and a potential signal for directing therapeutic strategies(21).
The majority of studies in the specialized literature unanimously support that sleep disorders constitute heightened risk factors for the development or exacerbation of symptoms associated with BMS. Consequently, from a medical practice perspective, this finding is valuable as the management of sleep disorders, coupled with the improvement of their quality, can provide significant benefits in alleviating symptoms related to BMS(22).
The significance of general conditions associated with BMS. A series of research studies suggest that associated general conditions may play a significant role in the genesis of manifestations in BMS. In this context, the specialized literature studies have identified several general conditions that appear to be involved in the development and exacerbation of BMS symptoms.
According to Klasser et al. (2011), there is a possibility that the preexisting systemic conditions in patients with BMS or even certain medications used to treat these conditions may be the cause or contribute to the onset of symptoms in patients with oral pain. A detailed analysis conducted at the University of Illinois at Chicago on a sample of 49 patients highlighted the following concurrent general conditions at the time of presentation, namely hypertension (33%), gastroesophageal reflux disease (29%), hypercholesterolemia (22%), autoimmune disorders (22%), thyroid disorders (14%), and anemia (2%)(15).
Association with stress. According to the study by Ohga et al. (2015), the etiology of BMS is unclear and multifactorial, likely involving complex interactions among peripheral, central, and/or psychogenic factors(23).
According to the analysis conducted by Spanemberg et al. (2015), among the possible causes of BMS, psychological factors such as stress, anxiety or depression can also be included(16).
In the same context, Demarosi (2013) acknowledges that most patients with BMS associate varying degrees of psychological disorders, including anxiety, depression, oncophobia, or hypochondria(3).
These psychological manifestations play a significant role in modulating pain perception, being capable of influencing the transmission of nerve signals from peripheral pain receptors to the central nervous system and altering the individual perception of pain. They can lower the pain threshold, causing ordinary stimuli to be perceived as painful(24).
Adamo et al. (2015) admit that stressful life events occupy a significant place in triggering nonspecific oral pain(5).
Although, initially, psychiatric illness was considered a primary cause of BMS, it is currently regarded as more of a concurrent or secondary factor, as there is no definite correlation between the onset of BMS and the stressful events reported by patients(10).
Prevalence of smoking. Smoking is not considered a predisposing factor for the onset or maintenance of specific symptoms. The majority of specialized studies do not view tobacco consumption as a contributing factor in BMS(24,25).
Contradictory data in the medical literature concerning the role of smoking in the etiopathogenesis of BMS continue to sustain its role in scientific debates. Proponents of smoking involvement in BMS pathogenesis attribute suffering to the actions induced by harmful substances, such as benzo(a)pyrene and cyclic aromatic hydrocarbons found in cigarette composition(13).
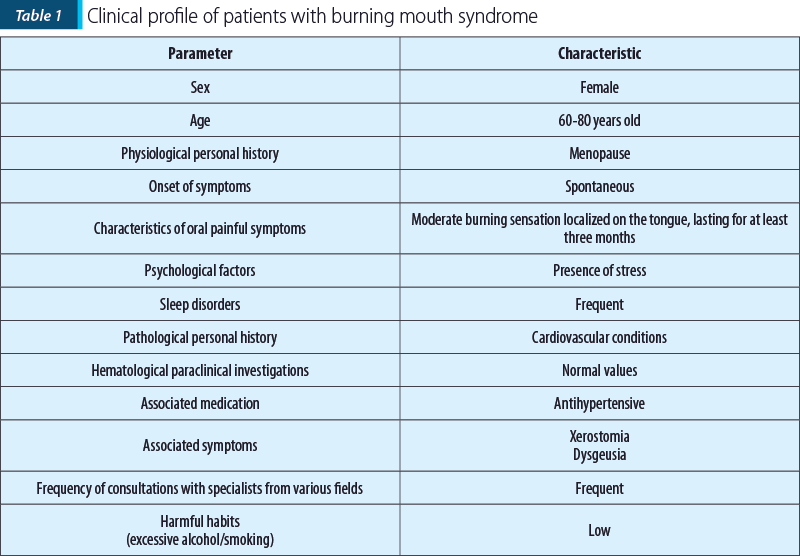
By integrating the data from the specialized literature, we sought to identify the possibility of outlining a distinct pattern predisposed to developing burning mouth syndrome (BMS). This pursued profile has been generically termed the “oral clinical profile” and is summarized in Table 1.
In conclusion, burning mouth syndrome is a complex condition characterized by the sensation of burning or pain in the oral cavity, and the clinical profile of a patient with BMS can be summarized in a set of specific characteristics. BMS primarily affects females, with a significantly higher prevalence around menopause. The average age of onset is around 60 years old. Psychological factors such as stress, anxiety and depression may play a role in triggering or exacerbating the BMS symptoms. Sleep disturbances are also common in patients with burning mouth syndrome. Burning mouth syndrome presents characteristic symptoms such as a moderate-intensity oral burning sensation, primarily localized on the tongue, lips and hard palate. The associated symptoms may include xerostomia and dysgeusia.
Patients with BMS seek the expertise of various medical specialists, including dermatologists, otorhinolaryngologists, psychiatrists and, additionally, other dental practitioners. Associations with general conditions such as hypertension, gastroesophageal reflux and thyroid disorders can contribute to the onset or exacerbation of BMS symptoms.
A multidisciplinary medical approach, along with collaboration between the physician and the patient, involving the provision of information about the condition and assurance of its benign nature, proves to be indispensable in addressing this condition.
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
- Adamo D, Spagnuolo G. Burning Mouth Syndrome: An Overview and Future Perspectives. Int J Environ Res Public Health. 2022;20(1):682.
- Scala A, Checchi L, Montevecchi M, Marini I, Giamberardino MA. Update on burning mouth syndrome: overview and patient management. Crit Rev Oral Biol Med. 2003;14(4):275-91.
- Ţovaru Ş, Ţovaru M, Demarosi F, Mihai L, Părlătescu I, Bold A, Gheorghe C, Vlădăreanu AM, Pitru A, Streinu-Cercel A, Coculescu E. Oral Medicine and Pathology – vol. II. Bucharest: Quintessence Publishing, 2015 [Romanian].
- Sardella A, Gualerzi A, Lodi G, Sforza C, Carrassi A, Donetti E. Morphological evaluation of tongue mucosa in burning mouth syndrome. Arch Oral Biol. 2012;57(1):94-101.
- Adamo D, Celentano A, Ruoppo E, Cucciniello C, Pecoraro G, Aria M, Mignogna MD. The Relationship Between Sociodemographic Characteristics and Clinical Features in Burning Mouth Syndrome. Pain Med. 2015;16(11):2171-9.
- Rodríguez-de Rivera-Campillo E, López-López J. Evaluation of the response to treatment and clinical evolution in patients with burning mouth syndrome. Med Oral Patol Oral Cir Bucal. 2013;18(3):e403-10.
- Mendak-Ziółko M, Konopka T, Bogucki ZA. Evaluation of select neurophysiological, clinical and psychological tests for burning mouth syndrome. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012;114(3):325-32.
- Sardella A, Lodi G, Tarozzi M, Varoni E, Franchini R, Carrassi A. Acupuncture and burning mouth syndrome: a pilot study. Pain Pract. 2013;13(8):627-32.
- Tammiala-Salonen T, Hiidenkari T, Parvinen T. Burning mouth in a Finnish adult population. Community Dent Oral Epidemiol. 1993;21(2):67-71.
- Gurvits GE, Tan A. Burning mouth syndrome. World J Gastroenterol. 2013;19(5):665-72.
- Tokura T, Kimura H, Ito M, Nagashima W, Sato N, Kimura Y, Arao M, Aleksic B, Yoshida K, Kurita K, Ozaki N. Temperament and character profiles of patients with burning mouth syndrome. J Psychosom Res. 2015;78(5):495-498.
- Klasser GD, Epstein JB, Villines D. Management of burning mouth syndrome.
- J Mich Dent Assoc. 2012;94(6):43-6.
- Gao J, Chen L, Zhou J, Peng J. A case-control study on etiological factors involved in patients with burning mouth syndrome. J Oral Pathol Med. 2009;38(1):24-8.
- Grushka M. Oral sensory phantoms and other strange phenomena, Conference of the “Carol Davila” University of Medicine and Pharmacy, 30 June 2014, Bucharest, Romania.
- Klasser GD, Epstein JB, Villines D. Diagnostic dilemma: the enigma of an oral burning sensation. J Can Dent Assoc. 2011;77:b146.
- Spanemberg JC, López López J, de Figueiredo MA, Cherubini K, Salum FG. Efficacy of low-level laser therapy for the treatment of burning mouth syndrome: a randomized, controlled trial. J Biomed Opt. 2015;20(9):098001.
- López-Jornet P, Camacho-Alonso F, Molino-Pagan D. Prospective, randomized, double-blind, clinical evaluation of Aloe vera Barbadensis, applied in combination with a tongue protector to treat burning mouth syndrome. J Oral Pathol Med. 2013;42(4):295-301.
- Baharvand M, Eshghpour M, Mortazavi H, Fallah Z. Comparison of burning mouth syndrome prevalence and its related factors between menopausal and non-menopausal women. J Dent Mater Tech. 2014;3:16-22.
- Spanemberg JC, Dias AP, Barreiro BOB, Cherubini K, de Figueiredo MAZ, Salum FG. Impact of burning mouth syndrome on quality of life. Rev Odonto Ciência. 2012;27(3):191-195.
- Grushka M, Epstein JB, Gorsky M. Burning mouth syndrome and other oral sensory disorders: a unifying hypothesis. Pain Res Manag. 2003;8(3):133-5.
- Chainani-Wu N, Madden E, Silverman S Jr. A case-control study of burning mouth syndrome and sleep dysfunction. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2011;112(2):203-8.
- Lee YC, Hong IK, Na SY, Eun YG. Evaluation of salivary function in patients with burning mouth syndrome. Oral Dis. 2015;21(3):308-13.
- Ohga N, Yamazaki Y, Sato J, Hata H, Murata T, Sakata K, Inoue T, Kitagawa Y. Dose escalation effectiveness and tolerability of paroxetine in patients with burning mouth syndrome and depressive conditions. J Oral Maxillofac Surg Med Pathol (Web). 2015;27(3):402-406.
- Minguez-Sanz MP, Salort-Llorca C, Silvestre-Donat FJ. Etiology of burning mouth syndrome: a review and update. Med Oral Patol Oral Cir Bucal. 2011;16(2):e144-8.
- López-Jornet P, Camacho-Alonso F, Andujar-Mateos P, Sánchez-Siles M, Gómez-Garcia F. Burning mouth syndrome: an update. Med Oral Patol Oral Cir Bucal. 2010;15(4):e562-8.
Articole din ediţiile anterioare
Algia bucală nespecifică – simptomatologie clinică
Actualitatea ştiinţifică şi importanţa pentru practica medicală a abordării acestei afecţiuni oro-dentale sunt susţinute nu numai de suferinţa pers...