Dentofacial esthetic rehabilitation in the anterior area of the dental arches is today a requirement without which social and professional integration is afflicted. Direct restorations with resin composites of carious and non-carious lesions can be achieved by different techniques, including the silicone index or silicone key method. This technique addresses the anterior teeth hard structure loss, involving the palatal surface, and it is performed with the help of a silicone index obtained from the impression of the affected area. The advantages of the silicon index method are, equally, the easy, morphologically and functionally correct reconstruction of the palatal contour and obtaining excellent restoration from an esthetic point of view, due to the possibility of layering the color shades of the used resin composite.
Anterior direct esthetic restoration using silicone index technique – case report
Restaurarea estetică directă în zona frontală prin tehnica cheii de silicon – prezentare de caz
First published: 24 mai 2024
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ORL.63.2.2024.9629
Abstract
Rezumat
Reabilitarea estetică dentofacială din zona anterioară a arcadelor dentare reprezintă astăzi o cerinţă fără de care integrarea socială şi profesională este afectată. Restaurările directe cu răşini compozite ale leziunilor carioase şi necarioase pot fi realizate prin diferite tehnici, între care şi metoda cheii de silicon. Această tehnică se adreseză pierderilor de substanţă ale dinţilor frontali ce implică faţa palatinală, realizându-se cu ajutorul unui index de silicon obţinut în urma unei amprente a zonei interesate. Avantajele tehnicii care utilizează cheia de silicon sunt în primul rând refacerea facilă, corectă morfologic şi funcţional a conturului palatinal, alături de obţinerea unor restaurări excelente din punct de vedere estetic, datorită posibilităţii de stratificare a nuanţelor de răşină compozită utilizată.
Introduction
Nowadays, esthetic demands of facial and smile aspect put a huge pressure on patients and, subsequently, on dentists. They are induced by socially promoted beauty standards, and while some have clinical justifications, as in case of dental restorations or orthodontic treatments, others go sometimes beyond real biological needs, and the bioethical aspects arise, as in case of cosmetic dentistry field(1).
Oral esthetic rehabilitation includes dental treatment of carious and non-carious lesions, especially when they are located in the anterior area of dental arches. There is a large number of direct and indirect treatment methods, which include: odontal restorations, resin composite/ceramic/zirconia veneers, ameloplasty, dental bleaching or microabrasion(2,3).
The direct resin composite restoration is the treatment of choice for hard tissues tooth loss, as a result of impressive development of these dental materials. They present esthetically outstanding properties, good biological tolerability, high bond strength, very good wear and mechanical characteristics, color stability, mimetic properties, and they permit easy working technique, with low costs. Being adhesive materials, resin composites are used in conservative dentistry approach, meaning a minimum sacrifice of sound tooth structure(4).
Silicone index direct restoration technique
Direct restorations can be done using different specific working techniques, depending on the area to which they address (anterior/posterior), the used materials (for example, sandwich technique with resin composite and glass ionomer cements), the quantity and volume of missing hard structure, or the number of involved tooth surfaces. For resin composites, the layering insertion methods provide very good results, both from an esthetic point of view (different shades can be applied alternatively) and from a functional point of view, because lowering polymerization shrinkage provide a better restoration longevity(5,6).
For the anterior area, the simple, very efficient and successful direct restoration technique using silicone index is recommended, especially when the esthetic demandings are high. It is also named as silicone-key or silicone-guided method. The clinical indications are dental caries, but they are frequently used for different coronal dental traumas like anterior teeth fractures. The silicon index or key is used to restore initially the palatal missing wall, and involves the mock-up method(7).
The cavity is initially restored with resin composites without using the adhesive system, the goal being only to provide a palatal surface similar to the neighboring teeth and in correct interdental contacts with the opposite arcade. If a previous restoration with a correct palatal morphology is present, it can be used for making the silicone guide/index. To obtain the guide, an impression is taken, and the first restoration is then removed. The silicone index is inserted and checked for adaptation in the oral cavity, and the direct restoration will start with modeling the palatal wall or the palatal shell. This stage is very easy to achieve when this method is used, because of the support the key provides for resin composite. After complete light curing and palatal anatomy are achieved, the next layers of resin composite are inserted(8).
The silicone index technique offers many advantages, such as: facile and low-time consuming restoration method, a global preview of the future anatomical and morphological characteristics of the restoration regarding shape, length and contour, easy functional restoration of palatal wall, in relationship with the opposite teeth, the material being kept by silicone index, and, finally, excellent esthetic results by layering resin composites of different shades. The final occlusal adaptation with burs is no longer needed, being replaced with just few adjustments with finishing and polishing instruments(9).
Case report
In this article, we present the treatment using direct silicone index or silicone-key method. A 26-year-old patient presented to dental practice for improving the esthetic aspect of smile. The patient was dissatisfied with the color, transparency and improper marginal adaptation of previous resin composite restoration in tooth 11. The restoration was placed about four years ago, using light curing resin composites, and the patient was happy with it but, gradually, the restoration’s characteristics have deteriorated, being considered inappropriate, especially given the fact that it was the only tooth restoration in the anterior area, all other teeth being intact and with a pleasant appearance regarding shape and dental arch alignment. Therefore, the patient decided to improve his dental aspect by replacing the old restoration (Figure 1).

The treatment started with professional brushing for removing the dental plaque and the extrinsic colorations from teeth surfaces. This aspect is extremely important especially in the case of restorations in the anterior area, where the first rehabilitation objective is the esthetic one. Also, in this regard, the proper color shades of resin composites have been established, using a shade guide.
The next step for this restoration technique is to obtain a silicone index/key, which is very important for the correct morphological and functional restoration of palatal tooth surface. This method is very useful especially when restoring extensive hard tissued loss, like anterior teeth injuries, when palatal structure, contour and shape of one or more teeth are missing. It was also proposed for tooth fragment reattachment(10,11).
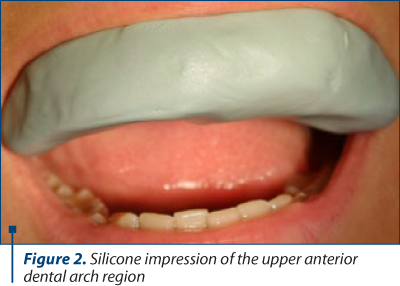
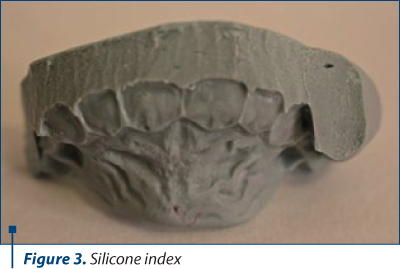
At the clinical examination, previously done when the patient had presented in our dental service, the palatal restoration wall was evaluated to be correct, and with good marginal adaptation, being used as a reference for the future coronal restoration. In order to obtain the palatal index, we took a putty consistency silicone material (ZetaPlus Putty, Zhermack) impression of the anterior area of upper dental arch and cutting it (Figures 2 and 3).
For the odontal treatment, the isolation was provided with a rubber dam. The previous restoration was removed, and the cavity walls were excavated for necrotic dentin. As we were restoring an anterior tooth, a 60° bevel in enamel was done at the cavosurface cavities margins, offering a gradual transition between the restoration and the tooth with an improved appearance, and, at the same time, a better retention and sealing for the future restoration(12).

The silicone index was inserted to check the proper adaptation prior to start the restoring therapeutic maneuvers (Figure 5). The cavity disinfection was done using 2% chlorhexidine.

For this case, we used Brilliant EverGlow® (Coltene), a submicron hybrid filler universal resin composite light curing restorative material, of the latest generation. We used A1/B1 and A2/B2 shades from Brilliant DuoShade system, which covers two VITA shades at a time, offering an excellent esthetic restoration as a result of special optical properties of this material, providing a harmonious matching with the surrounding tooth structure color. Its mechanical properties are very good, regarding bonding, low polymerization shrinkage and outstanding polishability, which is essential for obtaining a low surface roughness.
The total etch adhesive method was used, by applying 37% orthophosphoric acid both on dentin and enamel, 15 seconds for dentin and 30 seconds for enamel (Dental Etchant Etching Gel, Scotchbond, 3M ESPE). After completely washing of the acid, the cavity has been dried, and a universal adhesive system has been applied and light cured for 20 seconds (Single Bond Universal, 3M ESPE).
The restoration using silicone key method was accomplished by the initial reconstruction of the palatal wall, using the A2/B2 shade and light curing, followed by the insertion of the resin composite in the remaining hard tissues loss, in A1/B1 shade (Figures 6 and 7).


The occlusal adaptation was performed, with minimum adjustments needed, as a result of this technique, and the final aspect of the restoration was obtained after polishing with finishing and polishing instruments (Figure 8).
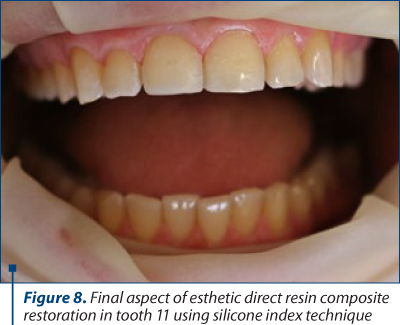
The patient considered the clinical result very good and satisfactory regarding the esthetic aspects of the restoration’s color, shade and transparency.
Conclusions
The silicone index or silicone key technique is a direct treatment resin composite option with many clinical advantages, being indicated for esthetically more challenging anterior restorations, when the use of different color shades allow obtaining a controlled opacity and translucency of restoration aspect. Another very important advantage is related to the accurate morphofunctional reconstruction of the missing hard dental structure, addressing especially to palatal area. Silicon index facilitates the easy, correct and predictable anatomical form of the palatal contour, thus a very good interdental contacts with the opposite arcade and with minimum adaptation. n
Acknowledgements. All the authors have equal contributions for this article.
Corresponding author: Sânziana Scărlătescu, e-mail: sanzianas@gmail.com
CONFLICT OF INTEREST: none declared.
FINANCIAL SUPPORT: none declared.
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
-
Prasad KN, Sabrish S, Mathew S, Shivamurthy PG, Pattabiraman V, Sagarkar R. Comparison of the influence of dental and facial aesthetics in determining overall attractiveness. Int Orthod. 2018;16(4):684-697.
-
Rani R, Chachra S, Sharma M, Bansal S, Kaur T, Sharma D. Simulating Natural Tooth Anatomy in Anterior Teeth Crown Fracture: A Case Report. Int Journal of Dent Res. 2019;4(2):38-39.
-
Gheorghiu IM, Mitran L, Mitran M, Iliescu AA, Perlea P, Scărlătescu S, Bucur F. Esthetic function direct restoration in the anterior area – case report. ORL.ro. 2023;61(4):41.
-
Staehle HJ, Wolff D, Frese C. More conservative dentistry: clinical long-term results of direct composite resin restorations. Quintessence Int. 2015;46(5):373-80.
-
Sadowsky SJ. An overview of treatment considerations for esthetic restorations: a review of the literature. J Prosthet Dent. 2006;96(6):433-42.
-
Shah YR, Shiraguppi VL, Deosarkar BA, Shelke UR. Long-term survival and reasons for failure in direct anterior composite restorations: A systematic review. J Conserv Dent. 2021;24(5):415-420.
-
Felippe LA, Monteiro S Jr, De Andrada CA, Ritter AV. Clinical strategies for success in proximoincisal composite restorations. Part II: Composite application technique. J Esthet Restor Dent. 2005;17:11-21.
-
Akbiyik SY. Restoration of Anterior Tooth Fractures Using Silicone Key Method: 3 Case Report. Int Arch Med Res. 2020;12(2):46-55.
-
Korkut B. Direct Esthetic Resin Restorations of Anterior Coronal Fractures: A Case Report. Brit J Med and Medical Res. 2016;17(10):1-5.
-
Romero MF. Esthetic anterior composite resin restorations using a single shade: Step-by-step technique. J Prostet Dent. 2015;114(1):9-12.
-
Alvares I, Sensi LG, Araujo EM, Araujo E. Silicone index: an alternative approach for tooth fragment reattachment. J Esthet Restor Dent. 2007;19(5):240-5; discussion 246.
-
Ramirez J. Esthetic Anterior Resin Restorations: To Bevel Enamel or Not?. Int J of Dental Sc. 2019;23(1):27-31.
Articole din ediţiile anterioare
Direct composite veneers for erosive-abrasive lesions – case report
Tratamentul leziunilor dentare abrazive şi/sau erozive este unul conservator. Una dintre metodele de tratament este faţetarea directă sau indire...
Restaurarea directă în zona frontală a distrucţiilor dentare coronare – prezentare de caz
Acest articol prezintă o temă de actualitate în domeniul medicinei dentare restaurative: restaurarea directă a distrucţiilor dentare coronare în...
Tratamentul leziunilor dentare necarioase
Leziunile dentare necarioase – fie că sunt cu sau fără pierdere de substanţă – conduc la apariţia tulburărilor fizionomice, având, de asemenea, un ...
Sensibilitatea postoperatorie asociată restaurărilor cu răşini compozite
În practica clinică ne confruntăm adesea cu durerea postoperatorie dentinară care apare după restaurarea directă coronară cu răşini compozite. Ar...