Authors have conducted a retrospective study based on the clinical experience of 93 patients admitted to IFACF-ORL ”Prof. Dr. D. Hociota” - Wards I between January 2010 and January 2015 for mucoceles with different localizations. A mucocele is defined as a mucous filled epithelium lined sac. Mucoceles are commonly caused due to obstruction of the drainage channel of paranasal sinuses. These expansive cystic masses are sometimes filled with mucopurulent secretions, sometimes associated bone destruction is also evident. The most frequent topography of mucoceles was in the paranasal sinuses: 38.6 % in the frontal sinus, followed by ethmoid sinus (24.7 % - the most uncommon locations were found in the medium and superior turbinate), maxillary sinus
(23.6 %), sphenoid sinus (13%) and early mucoceles (3.22 %). The elective radiological investigation in mucoceles is computed-tomography. Almost all surgeries were carried out under general anesthesia, performed with endoscopes, with which all relevant anatomical structures were visualized without difficulty. In conclusion, the endonasal marsupialisation technique is nowadays the surgical approach of choice in most cases.
Endoscopic approach of rinosinusal mucocele
Abordul endoscopic al mucocelului rinosinusal
First published: 15 mai 2015
Editorial Group: MEDICHUB MEDIA
Abstract
Rezumat
Autorii au realizat un studiu retrospectiv bazat pe experienţa clinică acumulată prin urmărirea a 93 de pacienţi internaţi în IFACF-ORL „Prof. Dr. D. Hociota” - Secţia I-IIA, între ianuarie 2010 şi ianuarie 2015 pentru mucocel cu multiple localizări. Mucocelul este definit ca o formaţiune saculară căptuşită de epiteliu ce conţine mucus. De obicei, mucocelele sunt datorate unei obstrucţii a canalelor de drenaj ale sinusurilor paranazale. Aceste mase expansive sunt uneori umplute cu secreţii mucopurulente, uneori asociate cu distrucţie osoasă. Cele mai frecvente localizări ale mucocelelor au fost în ordinea următoare: 38,6% la nivelul sinusului frontal, urmat de sinusul etmoid, cu 24,7% (cele mai rare localizări fiind aflate la nivelul cornetelor mijlocii şi superioare), sinusul maxilar cu 23,6%, sinusul sfenoid cu 13% şi mucocele la debut - 3,22%. Investigaţia de elecţie în diagnosticul mucocelului este tomografia computerizată. Toate operaţiile au avut loc sub anestezia generală, sub control endoscopic, cu ajutorul căruia s-au putut vizualiza structurile anatomice fără probleme. În concluzie, tehnica marsupializării este în ziua de azi metoda de elecţie în tratamentul mucocelului.
Introduction
Mucoceles of the paranasal sinuses were first described by Langenbeck (1820) under the name of hydatides. Rollet (1909) suggested the name mucocele (1). Sinus mucoceles are benign sinus tumors, defined as mucous filled epithelium lined sacs. These cystic masses are sometimes filled with mucopurulent secretions. Bone destruction may also be associated. It is an entity in which obstruction of the sinus cavity outflow tract, resulting in expansion of the sinus walls, has also been described. The histologic features are quite nonspecific, requiring clinical, radiologic, and pathologic correlations(2). Mucoceles may appear at any age and their incidence is similar for both, males and females.
The origin of sinus mucoceles remains controversial. Mucoceles are commonly caused by obstruction of drainage channels of paranasal sinuses. In this context, a hypothesis proposes that they appear due to a chronic inflammatory process occurring in a closed space(3). Other hypothesis is that they are caused by allergic sinonasal disease, trauma or prior sinus surgery, however, in many cases the cause remains unknown(4). Although conventional radiographies may give clues to the diagnosis of mucoceles, Computerized Tomographic (CT) scan and Magnetic Resonance Imaging (MRI) are radiologically superior in giving additional information of the presence, site, and extent of all paranasal sinus mucoceles.
The principal advantage of MRI over CT for sinus tumors is the ability of MRI to distinguish between tumor and obstructed sinus secretions and to assess the true extent of the tumor. There are three criteria for CT diagnosis of a mucocele: homogeneous isodense mass, clearly defined margin, and patchy osteolysis around the mass. Erosion of the sinus wall with marginal sclerosis is also an indicative finding. Typically, mucoceles tend to be fairly bright on T1Weight images compared to the brain and iso-hyperintense on T2Weight images. It is pathognomonic MRI finding for mucoceles(1). Mucoceles have thin peripheral linear enhancement whereas tumors have diffuse enhancement. No enhancement of the sinus secretions is seen on postcontrast images, except in the mucosa of the sinus, whereas tumors often enhance and show intermediate T2 signal, allowing differentiation of postobstructive secretions from tumor(6). The sagital and coronal planes are very helpful to evaluate cribriform plate extension; the coronal and axial planes are best to evaluate orbital, cavernous sinus. Differential diagnosis can be made with: idiopathic bone cavity (traumatic bone cavity, traumatic bone cyst, simple bone cyst, hemorrhagic bone cyst etc.), aneurysmal bone cyst mucus retention phenomenon (mucous retention cyst), cystic hygroma. As a particular case, by definition, a cyst will be considered to be a pathologic cavity at least partially lined by epithelium. To be an odontogenic cyst, the epithelial lining must be derived from odontogenic epithelium. As a particular case, by definition, a cyst will be considered to be a pathologic cavity at least partially lined by epithelium. To be an odontogenic cyst, the epithelial lining must be derived from odontogenic epithelium.
For the management of mucoceles the current trend was the endoscopic approach, while the external approach is reserved for a difficult or failed endoscopic approach, then a combined external and endoscopic approach is employed(5).
The aims of this study were to compare and describe the clinical characteristics of mucoceles occurring apparently with unknown cause vs. those occurring after sinus surgery; the complications following the sinus surgery and the rate of recurrence of mucoceles.
Materials and methods
This is an observational retrospective study based on our clinical experience on 93 patients admitted to IFACF-ORL „Prof. Dr. D. Hociotă” - Wards I, between January 2010 and January 2015, for different types of mucoceles.
All patients were subjected to common battery of tests including radiological evaluation using CT scan and/or MRI as and when required. Because MRI is primarily indicated for the evaluation of sinus tumors, and occasionally for inflammatory disease such as a mucocele, it was the imaging technique of choice, when possible, a standard head coil, with 3- to 5-mm slices.
Diagnostic nasal endoscopy was performed in all patients in order to confirm the diagnosis and to assess the extent. The exact surgical approach was determined on the basis of site, size, extent and preoperative diagnosis. Operative intervention was then carried out and the patients were followed-up over a period of 1 month, 3 months, 6 months, 1 year and then yearly and post-operative outcome was analyzed(7).
Most of the procedures were carried out under general anesthesia, performed with endoscopes with which all relevant anatomical structures were visualized without difficulty. Frequencies of topography, dimensions, clinical presentations and post-surgical complications of mucoceles have been reported.
Results
From the 93 patients enrolled, 46 were males. Mean age was 61 years (range: 16 to 77 years). In 2011 it was the largest number of mucoceles operated(27). The most frequent topography of mucoceles was in the paranasal sinuses (38.6% in the frontal sinus), followed by ethmoid sinus (24.7% - the most uncommon locations were found in medium and superior turbinate), maxillary sinus (23.6%), sphenoid sinus (13%) and early mucoceles (3.22%) (Table 1).
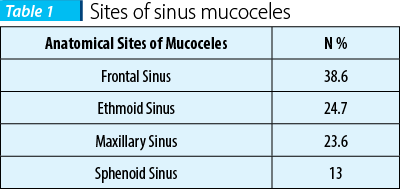
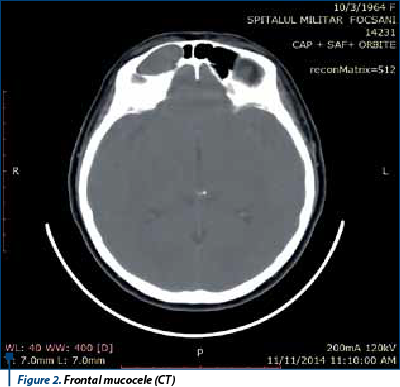
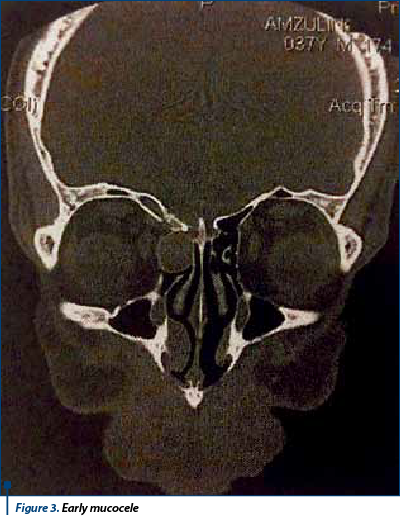
In our study mucocele of the frontal sinus is the most frequent one (38.6%) vs. ethmoid sinus (24.7%), maxillary sinus (23.6%), sphenoid sinus (13%) (Figure 1, Figure 2). Ethmoid sinus rate of complications is higher than in other sinuses that can move from cell to cell and can produce a bony defect on the lamina papyracea and displace medial rectus muscle laterally. In ethmoidal sinus, mucocele originate in one single cell, an early cell, which represents the point of extension of this pathology(8) (Figure 3, Figure 4).

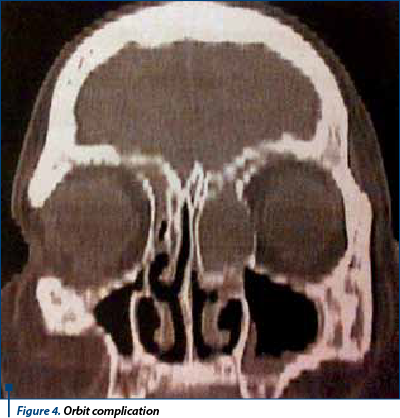
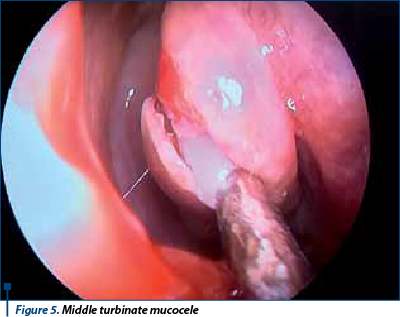
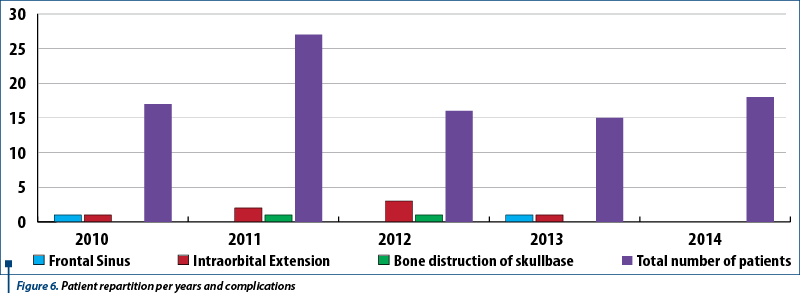
Concha bullosa is defined as aeration of the middle turbinate (Figure 5) that can be unilateral or bilateral. Aeration of the superior and inferior turbinates is less frequent. This illustrates that concha bullosa mucoceles could develop to such a massive extent that it leads to orbital complications (lamina papyraceea distruction with exoftalmy, limited eye movements, diplopia) and secondary frontal sinusitis in our series. A number of 11 patients developed immediate postoperative complications: intraorbital extension, frontal sinusitis, bone distruction of skullbase (Figure 6).
Simptomatology of the sphenoidal mucocele was represented mainly by important retroorbital pressure and pain. In some cases mucocele appeared in both sinuses and destroyed the intersphenoidal septum. The sphenoethmoidal recess may be blocked (Figure 7).

Discussions
The etiopathogenesis of mucocele is related to blocking of the sinusal ostium by healing fibrous and osteogenetic processes. Mucocele of the frontal sinus could also appear as a late complication of surgical intervention (Figure 1, Figure 2). Its symptomatology is clearly observed, the patient has a headache at any towards movement of the head. There are tardive complications that may appear because this involves bone distruction which happens after a longer time than the other sinuses. Frontal sinus is the only one which has two ways of drainage: by declivity and by mucociliary mucus. In case of a large frontal recess the opening of the ostium is easily performed, wheareas in case of a narrow frontal recess (“hourglass shape”) the opening implies some difficulties, always being available the risk of affecting the anterior ethmoid artery and penetrating the skullbase(8).
Like other aerated cells, the concha bullosa possesses a mucociliary transport system, with the ostium connecting sometimes the air cell lumen to the frontal recess(6). The air cavity in a concha bullosa is lined with the same epithelium as the rest of the nasal cavity, which can lead to involvement of these cells with the same inflammatory disorders experienced in the paranasal sinuses. Obstruction of the drainage of a concha can lead to mucocele formation.
The endoscopic mucocele marsupialization may be employed as an elective approach in all sinusal localizations, including those of the maxillary sinus. In order to form a continuous surface, the removal of the mucosal membrane could be, when possible, a part of the therapy(9).
Usually, diagnosis is made during the extension period and the related complications when the mucocele trespasses into the nearest district. In 10 patients, the case history was positive for odontoiatric surgery. All patients reported resolution of their symptoms, and in none of them was further surgery necessary(10).
Mucocele expansion occurs because of some factors, which include accumulation of inflammatory cells, fibrin, serum, and desquamated epithelial cells. As these products enter the cystic cavity, the accumulation of intraluminal products spurs the cystic expansion of the wall. Alternatively, cyst expansion may be spurred on by the inherent mitotic activity of the cyst wall itself. If this mitotic activity is the major component of the cyst expansion, it may be better to consider the lesion a cystic neoplasm rather than a simple cyst(6).
Since the ostial vicious circle “inflammation-obstruction” represents the primum movens, the traumatic event, surgical or accidental, which modifies the facial anatomic and functional conditions, causes mucocele formation(11). Of a great importance in mucocele pathology is the mucociliary clearance and apical junctional complexes between epithelial cells, which comprise a mechanical barrier between host and environment, and provides the first line of host defense for the nose and sinuses. Respiratory mucus traps foreign material and moves it out of the sinuses and nasal cavity toward the nasopharynx(6).
The surgical approach of sphenoid mucocele can be transseptal on the both sides for bilateral lesion, paraseptal (which is the most frequent one) and transethmoidal when there is simultaneous disease in the ethmoid sinus(8).
Conclusion
Mucocele is not a surgical emergency (with the exception of the complications) judging from the fact that it takes time for it to reach great dimensions and in clinical examination must be ruled out any cause of rhinological headache.
There have been presented some entities such as early mucocele and some rare cases of mucoceles of middle turbinate and superior turbinate.
Mucoceles mostly develop in the frontal sinus and less commonly in the ethmoid cell system or in the maxillary and sphenoid sinuses. The two most frequent causes of frontal mucoceles are: inflammatory changes and posttraumatic or post-interventional induced scarring of the nasofrontal duct after FESS(12).
In conclusion, the endonasal marsupialization technique is nowadays the surgical approach of choice in most of the cases. Immediate complications have not been reported but some tardive ones: mucocele recurrence in a small number of cases(6).
Bibliografie
-
Aggarwal, Sushil Frontal sinus mucocele with orbital complications: Management by varied surgical approaches. Asian J. Neurosurg. 2012 Jul-Sep; 7(3): 135-140.
-
Thompson, Lester Paranasal sinus mucocele. Ear Nose Throat J. 2012 July; 91(7): 276-278.
-
Devars du Mayne, M. Sinus mucocele: Natural history and long-term recurrence rate. European Annals of Otorhinolaryngology, Head and Neck diseases, 2012: 129, 125-130.
-
Lee, Khyung Comparison of Clinical Characteristics between Primary and Secondary Paranasal Mucoceles. Yonsei Med J. 2010 Sep 1; 51(5): 735-739.
-
Iseh, K. Endoscopic and External Surgical Approach to Paranasal Sinus Mucocele. J Surg Tech Case Rep. 2010 Jan-Jun; 2(1): 49–53,6. Flint, Paul Cummings Otolaryngology: Head and Neck Surgery, Philadelphia, Saunders, 2015: 117.
-
Jaswal, Abhishek Paranasal sinus mucoceles: a comprehensive retroprospective study in Indian perspective, Indian J. Otolaryngol. Head Neck Surg. April-June, 2008: 60, 117-122.
-
Budu, V. Chirurgia endoscopică rinosinusală, Editura Universitară “Carol Davila”, Bucureşti, 2014: p.
-
Budu, V. Chirurgia Etmoidului, Editura Universitară “Carol Davila”, Bucureşti, 2014.
-
Busaba, NY Endoscopic sinus surgery for inflammatory maxillary sinus disease. Laryngoscope 2002; 112: 1378-83.
-
Lory, D. Les mucoceles du sinus maxillare: a propos de trios cas. Revue Laryng 1987; 108: 71-6.
-
Constantinidis, J. Controversies in the management of frontal sinus mucoceles. Otorhinolaryngologia – Head and Neck Surgery Issue 42, October-November-December 2010: 8-14.
Articole din ediţiile anterioare
Mucocelul fronto-etmoidal exteriorizat - provocare diagnostică şi terapeutică
Mucocelul fronto-etmoidal este o patologie relativ rar întâlnită în practica ORL curentă. Cel mai frecvent, la prima prezentare la medic mucocelul ...
Mucocel de concha bullosa - rezolvare chirurgicală endoscopică
Cefaleea este o patologie redutabilă de graniță, cu care se confruntă medici de diferite specialități și care trebuie investigată minuțios în veder...
Marsupializarea endoscopică a mucocelului etmoidal
Mucocelul rinosinuzal se dezvoltă cel mai frecvent la nivelul sinusurilor etmoidal şi frontal. Diagnosticul de elecţie este imagistic – computer-to...
Mucocel etmoidal cu extensie orbitară – urgenţă medico-chirurgicală
Mucocelul sinusurilor paranazale a fost descris pentru prima dată în literatura de specialitate de către Langenbeck (1820) sub denumirea de „hidati...