The direct restoration of hard dental loss in posterior region presents both characteristics that come from the specifics of the dental caries in molars and premolars, as well as from the aspects of treatment techniques. The posterior area presents the highest incidence of dental caries mainly due to the teeth morphology (pits, grooves, cusps) and the consequences arising from this aspect. Regarding direct restoration of the teeth in the masticatory region, we are often confronted with difficulties and failures of the correct restoration of the interproximal contact area. Through detailed knowledge of the therapeutic protocol and properties of the materials, we can completely eliminate the failures of these restorations.
INTERDISCIPLINARY
Special aspects of direct restoration in posterior teeth
Particularităţi în restaurarea directă a dinţilor laterali
Irina-Maria Gheorghiu,
Loredana Mitran,
Mihai Mitran,
Sânziana Scărlătescu,
Alexandru A. Iliescu,
Paula Perlea,
Octavian-Andrei Nistor
First published: 28 septembrie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ORL.60.3.2023.8591
Abstract
Rezumat
Restaurarea directă a lipsei de substanţă în cazul dinţilor laterali prezintă atât particularităţi ce provin din specificul proceselor carioase de la acest nivel, cât şi din particularităţile tehnicilor de tratament. Zona laterală este zona ce prezintă cea mai mare incidenţă a cariei, în principal din cauza morfologiei dentare (şanţuri, fosete, cuspizi) şi a consecinţelor ce decurg din acest aspect. În ceea ce priveşte restaurarea directă, în mod deosebit în zona masticatorie, ne confruntăm cu dificultăţi şi eşecuri în refacerea corectă a ariei de contact, în cazul proceselor carioase proximale. Prin respectarea protocolului terapeutic şi ţinând cont întotdeauna de situaţia clinică globală a cavităţii orale, aceste manopere iatrogene pot fi evitate.
Introduction
Dental caries are one of the oldest diseases in the human race. People have been facing dental caries for thousands of years and, despite the evolution of science and the advances in dental medicine, the prevalence is still extremely high.
The most common dental condition and, as such, the reason for presenting to the dental office is represented by the pain caused by dental caries. Also, in our country, dental caries are considered to be one of the most common diseases of the dentomaxillary system, affecting 80-98% of the population(1).
The direct restoration of hard dental substance loss
The restorations in the lateral regions, namely class I and class II (the cavity classification according to G.V. Black), are particularly important from a functional and masticatory point of view, but also from an esthetic point of view, especially in mandibular teeth.
The correct restoration of the dental tissue loss through direct restoration is the essential criterion in modern dentistry. The posterior area presents the highest incidence of dental caries, mainly due to the teeth morphology (pits, grooves, accentuated cusps) and the consequences arising from this aspect. Also, being an area with a high functional importance, as mentioned before, during the trituration and fragmentation of food, traumatic injuries, such as cracks or coronal and coronoradicular fractures, may occur(2).
Modern dentistry requires materials that satisfy the patient’s needs, both from an esthetic criterion and also for the mechanical and biological properties. The resin composites are nowadays the election materials, with a wide variety of dental uses, including the restoration of teeth with various carious/noncarious etiology, hard dental loss, for teeth that have suffered traumatic injuries, or the immobilization of mobile teeth in periodontitis, but the dentist is the one who decides in which clinical condition are indicated and can be successfully used.
The most important current issue is the prevention of dental caries. Dental prophylaxis is the simplest and most accessible approaching method, but it is not so well known in our country, especially in rural areas, which is why the dentist must be the main messenger and promoter of dental prevention. Educating and informing patients about prophylaxis techniques is the dentist’s duty, who has to explain them the importance and benefits of an attitude of prophylaxis of oral cavity conditions – and primarily of dental caries, from which countless other local and locoregional complications arise, with influence in the entire body.
Countless studies have confirmed the increased prevalence of caries in the posterior teeth, both in the maxillary and the mandibular ones. The most affected are the first molars, in a percentage between 64.8% and 79.8%(3). The increased incidence of dental caries in these teeth is due to both dietary, economic and educational behaviors, respectively dental hygiene.
The posterior area is particularly vulnerable to caries due to the following aspects:
- the morphological complexity, especially of the occlusal face, the presence on the oral and buccal faces of the molars of fissures and pits, which cause the retention of food and microorganisms; also, a reduced thickness of the enamel at grooves site accelerates the dental caries evolution;
- the difficulty of performing a correct dental hygiene, as a result of a more restricted access, to which there can be added situations such as microstomia, limitation of mouth opening, and accentuated vomiting reflex;
- the proximal teeth faces, where cleaning and self-cleaning are difficult, benefit from a low saliva supply, also favoring the dental caries appearance;
- lack of education regarding the importance of dentition in the lateral area, even though the esthetic impact is not the main one, as in the frontal area; as such, patients brush their teeth more briefly, often partially ineffective. They also easily accept the loss of a molar or premolar as a result of dental caries complications in the posterior area.
The complexity of direct dental restorations in the posterior teeth
The direct restorations of the carious processes in molars and premolars present specific peculiarities, both because of the aspects related to their appearance and evolution, but also because of the technical aspects that complicate the treatment methods. Especially in the masticatory area we face difficulties and failures of the correct restoration of the interproximal contact area.
1. The characteristics of dental caries in the posterior teeth
First of all, due to its morphological aspect, the occlusal surface is the most susceptible to caries. Through the deposition and accumulation of bacterial microfilm, the phenomena of decalcification and demineralization of organic and inorganic dental structures are triggered(4). Teeth with deep grooves and pits are more susceptible to carious attack, as a result of more pronounced retention compared to those with an attenuated occlusal cusps and fissures (as it happens in the case of teeth with abrasion, for example). Therefore, an occlusal morphology with areas wider in surface than in depth is preferable. Dental areas with a greater susceptibility to caries are areas of chalky spots, demineralized areas, areas where the enamel is thin or deficient and exposed root surfaces. The latter frequently appear in the lateral area in teeth adjacent to the edentulous area, through the phenomena of vertical or horizontal migration.
The appearance of incipient caries in smooth surfaces and that on rough surfaces differs in the early stages: in smooth surfaces, the appearance of caries is of a triangle with the base facing outwards, while in occlusal surfaces, the appearance is in the form of two separate lesions at the level of the side walls of the pit, which converge when they reach the dentin-enamel junction. In the case of incipient caries located on the smooth, proximal surfaces of the posterior teeth, the bite-wing radiological examination is very useful, highlighting the incipient proximal lesions that exceed half the thickness of the enamel. In contrast, in the case of incipient caries in occlusal faces, the radiological examination doesn’t offer much information due to the complexity of this area, which can mask the incipient lesion(5).
2. Difficulties and failures in restoring the interproximal contact area in posterior teeth
Direct restorations of the posterior dental caries represent a challenge in many situations, especially if the proximal surfaces are involved. Before starting any treatment, the dentist must analyze all the potential risk factors, remove them or adapt his therapeutic behavior to the already existing situations. We refer to the complete occlusal analysis of the existing restorations on the opposing dental arch, the patient’s compliance with treatment, who must understand the need for restorations on both maxillary and mandibular teeth for correct mastication and ensuring the biological balance in the oral cavity, as well as maintaining proper hygiene. Sometimes, the option to perform a direct restoration for the missing dental substance in lateral area turns out to be incorrect, especially when it comes to a large missing tooth volume. In this situation, indirect restorations are the option of choice(6).
Unfortunately, therapeutic procedures are not always performed correctly, so they can be classified as iatrogenic procedures. These aspects appear when the work stages are not respected, which means a complete and thorough diagnosis, errors during the following of treatment protocol and, last but not least, the poor collaboration between the dentist and the patient. Regarding the restorations in the posterior teeth, the failures in the direct restoration of the interdental contact area can be classified as follows:
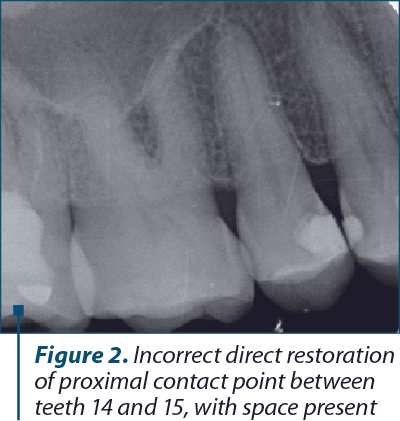
- Absence of proximal contact points with the existing space.
- Fracture of the marginal ridge or defective contours regarding the extension step of cavity preparation.
- Lesion of dental papilla from the incorrect use of the conformation system at the gingival threshold level.
- Incorrect preparation and insertion of the restorative material.
- Fracture of restorations or dental walls when the opposing arch was not properly analyzed, as well as parafunctions (bruxism).
- The use of incorrect techniques and materials whose validity period has passed, which no longer have the necessary properties to ensure a long-term restoration.
The most frequent mistake encountered in the restoration of approximal dental caries in posterior teeth is the appearance of interdental spaces at this level – i.e., the incorrect restoration of the contact point(7). As such, the patient will face complications in the short term (food retention, discomfort during mastication), but also later complications, by affecting the dental papilla. It will be traumatized by food contact, the gingival inflammation occurs and, over time, a localized gingival retraction appears, accompanied with bone resorption on the proximal tooth walls and dentin hypersensitivity(8).
In a class I cavity, where the proximal wall to be preserved is thin, its abolition is indicated, turning the cavity into a class II cavity, because the risk of this wall fracture is very high. We are in a similar situation when making massive direct restorations or not removing unsupported enamel prisms.
It is the responsibility of the dentist to use appropriate and in-date techniques and materials. Greater attention must be paid to cavities with radicular extension. In this situation, special sandwich treatment methods are indicated, due to the fact that the adhesion of the composite resins to the root cementum is poor(9).
The lack of correct marginal adaptation of the material can lead to secondary marginal caries. The situation occurs more frequently when interdental matrix bands and matrix holders are not used for proximal cavities. Also, when the principle of preventive extension is not respected, bacterial microfilm accumulates in the proximal cavity, which subsequently determines marginal nano-, micro-infiltration and secondary caries.
Therefore, the dentists’ main mistakes in direct restorations of dental caries in premolars and molars are: the incorrect use of proximal conformers and interdental wedges, the unsatisfactory restoration of the marginal ridge, the absence of finishing the restoration material after occlusal adaptation, improper treatment technique (for example, stratified layering or sandwich techniques, each for special clinical cases)(10). Unfortunately, iatrogenic maneuvers of this type are encountered with a high frequency in dental offices, but following the therapeutic protocol and always taking into account the entire situation of the oral cavity, they can be avoided.
Last but not least, the patient is responsible for complying with the indications received from the dentist, regarding the complete and complex restoration of the oral cavity, as well as maintaining proper hygiene, to ensure an increased life span of the direct restorations in the posterior teeth(11).
Conclusions
The direct restoration of hard dental loss in the posterior region presents both characteristics that come from the specifics of the dental caries in molars and premolars, as well as from the specific aspects of treatment techniques. Even though this area is given less importance from an esthetic point of view, it is mandatory to be properly restored due to the subsequent local and locoregional implications and repercussions. The most frequent mistakes encountered are related to the proximal cavities and the need to restore the interproximal contact area, but a thorough knowledge of the techniques and properties of the materials can completely eliminate the failures of these restorations.
Acknowledgements: For this article, all the authors have equal contributions.


Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
- Bîcleşanu C. Diagnosticul şi managementul modern al cariei dentare. Craiova medicală. 2008;10(3):178-182.
- Zabrovsky A, Mahmoud R, Beyth N, Ben-Gal G. Direct Posterior Restorations: A 13-Year Survey of Teaching Trends and Use of Materials. Oper Dent. 2018;43(6):E273-E279.
- Hyunseok L, Soyoun A. Caries prevalence by risk factor and tooth type using DMFT-related indices. J Korean Acad Oral Health. 2020;44(4):187-193.
- Carvalho JC, Dige I, Machiulskiene V, Qvist V, Bakhshandeh A, Fatturi-Parolo C, Maltz M. Occlusal Caries: Biological Approach for Its Diagnosis and Management. Caries Res. 2016;50(6):527-542.
- Janjic Rankovic M, Kapor S, Khazaei Y, Crispin A, Schüler I, Krause F, Ekstrand K, Michou S, Eggmann F, Lussi A, Huysmans MC, Neuhaus K, Kühnisch J. Systematic review and meta-analysis of diagnostic studies of proximal surface caries. Clin Oral Investig. 2021;25(11):6069-6079.
- Vetromilla BM, Opdam NJ, Leida FL, Sarkis-Onofre R, Demarco FF, van der Loo MPJ, Cenci MS, Pereira-Cenci T. Treatment options for large posterior restorations: a systematic review and network meta-analysis. J Am Dent Assoc. 2020;151(8):614-624.e18.
- Bărbuceanu L, Gheorghiu IM, Perlea P, Mitran L, Mitran M, Iliescu AA. The Use of UnimatrixR Matrix System for Restoration of Interdental Contact Points – Case Report. ARS Medica Tomitana. 2019;25(4):157-160.
- Peumans M, Venuti P, Politano G, Van Meerbeek B. Effective Protocol for Daily High-quality Direct Posterior Composite Restorations. The Interdental Anatomy of the Class-2 Composite Restoration. J Adhes Dent. 2021;23(1):21-34.
- Thalacker C. Dental adhesion with resin composites: a review and clinical tips for best practice. Br Dent J. 2022;232:615–619.
- Kaisarly D, Gezawi ME. Polymerization shrinkage assessment of dental resin composites: a literature review. Odontology. 2016;104(3):257-70.
- Borgia E, Baron R, Borgia JL. Quality and Survival of Direct Light-Activated Composite Resin Restorations in Posterior Teeth: A 5- to 20-Year Retrospective Longitudinal Study. J Prosthodont. 2019;28(1):e195-e203.
Articole din ediţiile anterioare
INTERDISCIPLINARY | Ediţia 4 61 / 2023
Esthetic function direct restoration in the anterior area – case report
Irina-Maria Gheorghiu, Loredana Mitran, Mihai Mitran, Alexandru A. Iliescu, Paula Perlea, Sânziana Scărlătescu, Florin Bucur
Restaurarea cu succes a funcţiei fizionomice a zonei anterioare a arcadelor dentare impune ca medicul dentist să aibă cunoştinţe avansate despre ...
24 noiembrie 2023
INTERDISCIPLINARY | Ediţia 4 45 / 2019
Restaurarea directă în zona frontală a distrucţiilor dentare coronare – prezentare de caz
Irina-Maria Gheorghiu, Loredana Gheorghiu, Mihai Mitran, Sânziana Scărlătescu, Dr. Alexandru Iliescu, Paula Perlea
Acest articol prezintă o temă de actualitate în domeniul medicinei dentare restaurative: restaurarea directă a distrucţiilor dentare coronare în...
13 decembrie 2019
INTERDISCIPLINARY | Ediţia 1 62 / 2024
Restaurările estetice adezive directe în zona laterală
Irina-Maria Gheorghiu, Loredana Mitran, Mihai Mitran, Octavian-Andrei Nistor, Alexandru A. Iliescu
Acest articol prezintă caracteristicile restaurărilor estetice realizate cu materiale aderente la nivelul dinţilor laterali. Sunt prezentate ma...
20 februarie 2024