Healthcare professionals are confronted with multiple stressors in their daily practice and data from the literature support a higher incidence of stress-related disorders, as well as isolated symptoms of such disorders in physicians and auxiliary personnel than in the general population. The current pandemic increases not only the workload for these professionals, but also their risk to suffer from other possible stressors (e.g., worries about loss of personal health or fear to contaminate family members, facing misconceptions in the general population about the pandemic that may translate in a suspicious or even aggressive attitude toward physicians, periods of isolation secondary to work-related tasks, worries about their own lack of professional efficiency due to exhaustion, changes in personal lifestyle and daily routines, insufficient information about the new type of coronavirus, worries about the quality of the protective equipment etc.). All of these factors may lead to a higher rate of professional stress-related disorders in time of pandemic than during common working periods. Burnout syndrome, adjustment disorders, major depression, posttraumatic stress disorder, acute stress reaction and substance use disorders are expected to be reported more frequently in healthcare professionals, based on the analysis of data collected during previous epidemiological crises worldwide. Therefore, programs for prevention, early detection, and treatment that target healthcare professionals are recommended, and education about mental health should be actively promoted in this population.
Aspecte de diagnostic şi tratament al tulburărilor asociate stresului profesional la personalul medical în contexul pand
Diagnostic and treatment features of work stress-related disorders in healthcare professionals in the context of COVID-19 pandemic
First published: 30 septembrie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Psih.65.2.2021.5372
Abstract
Rezumat
Profesioniştii din domeniul sănătăţii se confruntă cu numeroşi factori de stres în practica de zi cu zi, iar datele existente în literatură arată o incidenţă mai mare a tulburărilor legate de stres şi a simptomelor izolate asociate acestora în cazul medicilor şi al personalului auxiliar, comparativ cu cea din populaţia generală. Pandemia actuală conduce nu doar la creşterea volumului de muncă pentru profesioniştii din sănătate, ci şi la nevoia acestora de a face faţă altor factori de stres, cum ar fi îngrijorările legate de sănătatea proprie şi de riscul de a-i contamina pe cei apropiaţi, lipsa de cooperare sau chiar agresivitatea unor pacienţi care nu înţeleg riscurile asociate acestei infecţii, perioade de izolare impuse de activitatea profesională, teama de scăderea performanţelor profesionale din cauza oboselii, schimbări ale stilului de viaţă impuse de pandemie, informaţii insuficiente despre noul tip de coronavirus, griji legate de calitatea materialelor de protecţie etc. Toţi aceşti factori pot conduce la rate mai mari de tulburări legate de stres la profesioniştii din sănătate aflaţi în prima linie. Sindromul de burnout, tulburările de adaptare, depresia majoră, tulburarea de stres posttraumatic, reacţia acută de stres şi tulburările legate de consumul de substanţe au fost raportate în literatură ca fiind mai frecvent întâlnite la medici şi la personalul auxiliar, în condiţiile unor situaţii de criză epidemiologică majoră. Din acest motiv, se impune elaborarea unor programe dedicate prevenţiei, recunoaşterii precoce şi terapiei adecvate în cazurile de patologie legată de stresul profesional la cei care lucrează în prima linie a combaterii pandemiei. Informarea adecvată legată de semnele acestor tulburări trebuie, de asemenea, promovată la nivelul profesioniştilor din sănătate.
Introduction
Mental disorders related to professional activity have been defined by the World Health Organization (WHO) as “multifactorial diseases which may frequently be work-related, but also occur among the general population. (…) They may be partially caused by adverse working conditions, aggravated, accelerated or exacerbated by workplace exposures, and they may impair working capacity”(1). Under the COVID-19 pandemic conditions, the pressure on healthcare professionals has increased sharply, a phenomenon which requires increased attention in order to actively prevent and early intervene in new-onset stress-related disorders. A continuous increase of the professional tasks, changes of the work regimen (night shifts, extended program to face new challenges), the fear of getting infected or infecting one’s relatives, the stress of quarantine in case of contamination, all these factors and many others fundamentally changed the paradigm of psychiatric and psychological care in the context of the pandemic. Therefore, doctors and support staff themselves have become a vulnerable population which requires close health monitoring. As a consequence of these factors, the appearance within the medical staff of both stress-related disorders and isolated psychiatric symptoms has been reported in the context of epidemiological crises. Thus, a study conducted during a pandemic reported a high incidence of physical asthenia, anxiety, various emotional disorders, or sleep disorders in healthcare workers(2). In a recent study (N=1953 healthcare professionals), the most frequently reported psychiatric manifestations were depressive symptoms (approximately 50.7%), anxiety (approximately 44.7%) and sleep disorders (approximately 36.1%)(2). Posttraumatic stress disorder, major depression, anxiety disorders and burnout syndrome have been reported by medical staff after the completion of other pandemics(2,3).
Among the most frequently cited risk factors associated with the occurrence of stress disorders in healthcare professionals in the context of COVID-19 pandemic are female gender, middle-level professional status, low social support, and concerns about their own or close relatives contamination/illness(4). The current pandemic is an independent risk factor for stress-related disorders, due to the anxiety-saturated social climate and the general insecurity it perpetuates, even among doctors and support staff(5). Organizational factors related to the practice of the medical profession in a new domain (by recruiting medical staff without previous experience in the field of infectious diseases for duties within the COVID-19-specialized hospitals), the scarcity of protective materials or lab tests for SARS-CoV-2 infection, the lack of pathogen-specific drugs, social stigmatization of COVID-19-positive patients, all these factors lead to additional pressure on healthcare professionals(5).
Main disorders associated with occupational stress in the context of COVID-19 pandemic in medical staff and appropriate evidence-based treatments
From the wide range of disorders correlated with high occupational stress, we selected burnout syndrome, major depression, adjustment disorders, acute stress reaction, posttraumatic stress disorder, and substance use disorders. The analyzed data come from epidemiological and clinical studies that included: (1) healthcare professionals during an epidemiological crisis; (2) healthcare professionals in normal working conditions; (3) the general population exposed to significant stressors, where no studies focused on healthcare professionals could have been detected (for example, for some forms of therapeutic intervention).
Burnout syndrome
The term burnout was coined by the American psychologist Herbert Freudenberger in the 1970s, in order to describe the consequences of severe stress and of too high self-imposed goals for professionals in areas involving the assistance of other people(7). Subsequently, the conceptual sphere of “burnout” expanded, and this syndrome is no longer limited to a certain professional category(6). In the medical field, burnout is especially relevant due to the difference between systemic demands and individual resources, a phenomenon that leads to exhaustion and reduced professional performance(7,8).
This pathology has an estimated prevalence among physicians that varies significantly, from 0% to 80.5%, according to a systematic literature review that included 182 studies with 109,628 participants from 45 countries(9). This wide variation in prevalence has been explained by the different studies design, lack of homogeneity of the diagnostic criteria, and different statistical methods used for data processing(9). Burnout was also reported by nurses, and its presence was inversely proportional to the degree of patients’ satisfaction with the received care(10). Also, an important risk for this syndrome onset is reported by psychologists and psychotherapists(11).
Burnout syndrome predicts the onset of depressive symptoms, dissatisfaction with own life, use of psychotropic medication, hospitalization for a mental disorder, lack of fulfillment at work, absenteeism, and disability retirement(12,13). The same syndrome is an important predictor of hypercholesterolemia, type 2 diabetes, ischemic coronary heart disease, hospitalizations for cardiovascular disease, musculoskeletal pain, changes in pain perception, prolonged fatigue, headache, gastrointestinal dysfunction, severe respiratory problems, and even premature death(13).
The key elements of burnout are emotional exhaustion, depersonalization, and lower level of personal achievement, while some authors consider this syndrome to be a type of depression rather than a distinct clinical entity(14). Thus, exhaustion is manifested by an inability to cope with everyday situations, feeling tired and lacking energy; depersonalization is accompanied by cynicism and a hypercritical attitude towards colleagues and the workplace, as well as an emotional detachment from others; reduction in the accomplishment of daily tasks is manifested in all areas (e.g., professional, family and social), with a decrease in the patient’s creativity and difficulties concentrating(6). According to ICD-10, the burnout syndrome, coded Z73.0, is placed in the category of “Problems related to life management difficulties”(15). In ICD-11, burnout syndrome is considered an occupational phenomenon, not a medical condition, and it is included in the chapter “Factors that influence health or involve contacts with health services”(16). The definition of this syndrome in ICD-11 mentions the existence of three dimensions: the feeling of lack of energy, or exhaustion; increasing mental detachment from one’s job, negativity or cynicism related to professional aspects; low professional efficiency(16).
The Maslach Inventory for Burnout is the most validated instrument for assessment of the severity of this syndrome and it includes items distributed on the three dimensions previously mentioned: exhaustion, depersonalization or cynicism, and dissatisfaction in the professional domain(17). This instrument consists of 22 items scored on a 7-point Likert scale, depending on the symptoms' frequency(17).
Cognitive-behavioral therapy has led to improved emotional exhaustion in several clinical trials(18). Coping skills training – for example, by practicing conflict resolution techniques, effective time management, assertive training, as well as learning relaxation techniques could be useful in the treatment of burnout, but also in preventing its onset(19,20).
Other investigated treatment methods were meditation techniques (yoga, mindfulness), interventions to stimulate participation in group activities and music therapy, but the level of evidence in their favor is low(18,21).
Structured physical exercise for therapeutic purposes could be beneficial in patients with burnout syndrome, and some authors believe this could distract patients from stressful situations and mitigate the psychological impact(22). Exercise could increase the feeling of self-efficacy and even reduce the physiological sensitivity to chronic stressors(22,23). Consequently, exercise therapy could be a useful option, although a meta-analysis that included four studies focused on this type of intervention did not detect significant differences from the control group(24).
Interventions at an organizational level to address the causes of occupational stress, targeting the management of those units (hospitals, day-care units etc.), could lead to favorable long-term effects for patients with burnout(25). Such methods are the restructuring of professional tasks (by decreasing the daily workload, longer breaks), increasing the degree of personnel participation in the decision-making process, increasing the sense of control over professional tasks for each member of the team etc.(25,26)
Regarding the occurrence of this syndrome in mental health specialists, it should be mentioned as causal factors their involvement in caring for patients who have suffered psychological trauma and the possible onset of phenomena such as “compassionate fatigue”, “secondary traumatic stress” or “induced trauma”(27). Other factors, like the negative transference – directing the anger and even the aggression of some patients to the attending physician or the psychiatrist’s feelings of helplessness in the face of patients’ distress can also contribute to the appearance of burnout syndrome(28).
Several recommendations for mental health professionals in order to prevent the burnout onset are: increase the level of support (formal, from colleagues, use of community resources), the frequent assessment of the assigned professional tasks, in order to ensure there are no redundancy of the risk factors, diversifying the style of professional activity or involvement in extraprofessional activities (hobbies, personal interests), and timely processing of personal traumas, especially in the case of specialists working in the field of palliative care or psychotraumatology(20).
Depressive disorders associated with professional activity-related stress
Depressive disorders induced by occupational factors – such as increased demands, reduced control over assigned tasks, lack of gratification, interpersonal conflicts, role-associated stress and social isolation – may be detected by both reduced professional performance and direct reporting(29). Due to the common causal factors and symptoms partial overlap, sometimes the distinction between burnout and depression is difficult to achieve(29).
An association between occupational stress severity and the onset of major depressive episodes has been reported in large-scale epidemiological studies, such as the Canadian Community Health Survey(30). Excessive stress was associated with depression, especially in men, and the lack of social support correlated with depression in both sexes, while women who had a lower level of professional decision-making were at higher risk for depression, compared to women in higher decision-making positions(30). According to these data, primary prevention and treatment strategies should be adapted to specific organizational factors(30).
A study from Germany revealed that 17% of the resident doctors interviewed (N=435) had a high degree of occupational stress and 9% reported a high level of depressive symptoms(31). The highest level of emotional stress was reported by resident pediatricians, followed by neurologists, internists and gynecologists, while occupational distress level was self-assessed as high by resident surgeons(31).
According to a meta-analysis, depression and burnout syndrome overlap in clinical research (r=0.52, CI=0.49-0.54), but when specific tests were used to measure the severity of burnout or when the study design was of higher quality, the strength of the association between the two disorders was less significant(19). This suggests that depression and burnout are different constructs, describing distinct pathologies, which may occasionally overlap in the same person(32). Some symptoms are common to depression and burnout syndrome (for example, fatigue, decreased feelings of usefulness, increased feelings of helplessness), but there are also important differences: in depressive patients, the perceived lack of efficacy does not refer only to the professional tasks; there is a significant lack of hope, suicidal ideation may appear etc.(6) Although patients with burnout may be distinguished on the basis of clinical manifestations from those with major depression, it is possible that the former may increase the risk of developing a mood disorder, which recommends an active monitoring of these people, using validated psychometric tools(6).
The prevalence of major depression in primary care staff was considerably higher than that observed in the general population, in an epidemiological survey conducted in the city of São Paulo (16% versus 9.4%)(1). The longer duration of activity in that service, the lack of feedback from superiors on his/her performance, and lower levels of social support from colleagues and supervisors correlated with higher rates of depressive symptoms and major depression(1).
Suicide is a complication of the depressive disorder and it has been reported to have a high rate of occurrence in physicians compared to the general population(33). This rate is increased in both women and men, and access to lethal means and medical knowledge causes the percentage of completed suicide to be high(33). It is estimated that one million patients lose their doctor each year due to suicide, and almost 400 doctors commit suicide annually (the rate may be higher due to under-reporting)(33).
Regarding the estimation of the depressive disorder and depressive symptoms prevalence in residents of different specialties, meta-analyses revealed an average of 28.8%, with values between 20.9% and 43.2%, depending on the tool used and the year of the residents training (the percentage increases in the last years of residency)(34). No differences were identified according to this meta-analysis between residents in medical versus surgical specialties, or between longitudinal versus transverse studies(34). Other studies have shown that, in general practitioners (GPs), the usual administrative tasks, daily job requirements, interference of work with family life and interruptions during professional activity reduce their psychological well-being(35). In anesthesiologists, the communication within the hospital and the perceived control over professional tasks were significant in determining the professional satisfaction and psychological well-being(36).
The therapeutic interventions in these cases were divided into primary (structural or organizational changes), secondary (stress management or coping skills training) and tertiary (targeting patients with stress-induced mental disorders)(37-39).
From the category of tertiary interventions, interpersonal therapy can be useful in the case of depression associated with professional activity, starting from the vulnerability-stress diathesis and the fact that medical activity involves functioning in an interpersonal context(29).
Physicians who received prolonged medical leave (over 90 days), who had a diagnosis of depression induced by occupational activity, dysthymia or maladaptive stress reactions were treated with group cognitive therapy, group psychodynamic therapy, or were part of the control group, according to a longitudinal study(40). At 12 months after the end of therapy, 70% of participants met the criteria for a significant change in depressive symptoms, while other variables monitored also improved, without significant differences between the three groups(40).
Mindfulness therapy could be an option for the prevention of depression and burnout in healthcare professionals, according to a longitudinal, randomized study that included 288 students in Medicine and Psychology from Norway, who followed a seven-week program of mindfulness-based training(41). After six years from the end of the training, it was observed that the well-being was increased in the people who followed this program, compared to those who did not follow it, which correlated with an increase of the problem-focused coping and decrease of the avoidance-focused coping(41).
Because no specific recommendations on the pharmacological therapy of major depression associated with occupational stress have been detected in the literature, and because there are no controlled studies on this population, the therapeutic management will follow the same principles as for any other major depressive episode in the general population. Additional precautions related to the impact of medication on cognitive functions will be considered, given that we are talking about an active population, involved in stressful daily professional activities.
An important aspect in these cases is early detection, in order to prevent severe complications (e.g., suicide or the onset of a substance-related disorder). Screening programs for major depression in vulnerable populations, exposed to important stressors related to the professional environment, especially during the COVID-19 pandemic, should become an important part of the psychiatric and psychological care. Screening and early detection can have favorable effects reflected in decreasing excessive involvement (defined as working overtime under significant stress), absenteeism, extended leave from work, accidents at work, decreased quality of life, and occurrence of organic or psychiatric pathologies associated with persistent stress(42).
Adjustment disorder
This pathology is associated with the action of acute and chronic stressors and has been present as diagnosis since the DSM III(43). According to the latest edition of DSM, the adjustment disorder is reactive to a stressor that has appeared in the last three months, has a significant functional impact, and its duration is limited to six months(44). However, if the stress factor or its consequences persist, the adjustment disorder may also continue(44).
In ICD-11, this pathology is defined as “maladaptive reaction to an identifiable psychosocial stressor or to multiple stressors” that usually occurs within one month after the trigger occurred(45). ICD-11 also mentions that the patient is concerned about the stressor or its consequences (e.g., excessive worries, recurrent and painful thoughts related to the stressor, constant ruminations about its consequences), the failure to adapt to stressors causing significant dysfunction in personal, family, social, educational or occupational life(46). The disorder usually resolves within a maximum of six months, unless the stressor persists beyond this period(45).
There are some debates about the validity of this diagnosis, its critics mentioning the lack of specifics regarding the nature or severity of the stressor and the type of dysfunction associated with symptoms in the current classifications, as well as the lack of validated diagnostic and monitoring tools(47,48).
Adjustment disorder may be associated with an increased suicide risk compared to the general population, some studies showing that behavioral symptoms and chronicity are the strongest factors of negative prognosis(49,50). Studies that included five-year follow-up visits revealed that 5% of patients had at least one suicide attempt(49).
A retrospective study (N=100 patients diagnosed with adjustment disorder) showed that a higher quality of rehabilitation and its continuity correlated with a shorter duration until partial/complete resuming of activity, independent of other performance indicators(50). Because adjustment disorder is the result of an interaction between a stressor and a certain psychological vulnerability, it is necessary to analyze the characteristics of the professional environment/specific working tasks and the personality profile of each individual. The occupational physician, the psychiatrist, the clinical psychologist and the specialist in organizational psychology should work together to identify the causes of work-related adjustment disorder(51).
Solution-focused psychotherapy, which trains the patient in solving current problems and in developing effective coping mechanisms for facing various stressors similar to those that triggered the current disorder, could be the optimal solution for these patients(52). Interpersonal therapy and solution-focused therapy are both cited as possible effective strategies in this disorder(52).
According to a meta-analysis that integrated 29 studies focused on pharmacological and psychosocial interventions in adjustment disorders, cognitive-behavioral therapy, psychodynamic-oriented therapies, behavioral therapies and relaxation techniques were the most intensively studied for this indication(53). Real time-administered or online-administered individual cognitive-behavioral therapy proved to be significantly superior to the waiting list, and the online version led to greater improvements on the long term(54).
From a pharmacological point of view, tianeptine, selective serotonin reuptake inhibitors, trazodone, S-adenosyl-methionine, lormetazepam, etifoxine and alprazolam were studied for this pathology, but the trials quality was considered low, therefore no such treatment could be recommended with certainty based on the available evidence(53).
Acute stress reaction and posttraumatic
stress disorder
Stress-related disorders have been associated by several studies with the medical profession, but their prevalence in clinical practice is underestimated(55). Thus, some studies suggest these disorders are more commonly diagnosed in physicians than in the general population in the USA, and the most vulnerable occupational categories would be: emergency physicians, doctors working in isolated areas, residents, trainees, doctors involved in malpractice lawsuits, doctors who are indirectly exposed to trauma (“secondary victims”)(55). In addition, the cumulative stress of medical practice can cause symptoms that are specific to this pathology(55).
An epidemiological study involving US resident physicians showed that the incidence of posttraumatic stress disorder (PTSD) is higher in this occupational category than in the general population, and the most common causes cited were violence, death of their patients, bullying and medical errors(56).
In Europe, an epidemiological study found that one in three emergency physicians had subclinical levels of anxiety and 14.5% had a clinical level of PTSD, while the level of fatigue was high, but not directly correlated with traumatic events and occupational risks(57). According to the diathesis-stress model, the individual vulnerability factors are important in the PTSD onset. For example, in a population exposed to a high level of stress, only 3.5% had symptoms of PTSD, suggesting the involvement of other factors in the etiology of this disorder, in addition to the immediate stressor(58).
PTSD can reduce the professional performance of physicians, and a study comparing coping skills, burnout rate and acceptance of therapy in doctors with PTSD and those without this diagnosis revealed that PTSD was associated with significantly more anxiety, depression, negative coping strategies, burnout and refusal to accept the recommended treatment(59).
In the context of the current pandemic, some researchers estimate, based on the data analysis derived from other epidemiological crises, a risk for PTSD in frontline healthcare professionals of over 10%(60). The same authors recommended psychotherapy or counseling sessions for frontline medical staff, without prior planning (“drop-in sessions”), either in physical format or online(60). Other studies reported higher incidences of PTSD in medical staff, based on the analysis of data from the SARS (2003) or H1N1 (2009) epidemics and from physicians caring for HIV patients, with rates reaching 21% (10-33%), while 40% of them reported signs of PTSD even three years after exposure to the work-related stressful event(61,62).
Unlike the adjustment disorder, in the case of the acute stress reaction (ASR) it is necessary the presence of specific symptoms between three days and one month after the triggering event(44). For PTSD, a period of at least one month from the traumatic event is required(44). The sets of symptoms needed to establish the diagnoses of ASR and PTSD are different from the criteria needed to diagnose an adjustment disorder(44).
In terms of treatment, PTSD benefits from high-level recommendations for cognitive processing therapy, prolonged exposure therapy, trauma-focused cognitive-behavioral therapy, short eclectic therapy, desensitization therapy and eye movement reprocessing (EMDR)(63-65). The pharmacological approaches to this pathology include: selective serotonin reuptake inhibitors (especially sertraline and paroxetine, but also fluoxetine) – however, the risk of relapse after stopping these agents is quite high; serotonin and norepinephrine reuptake inhibitors; trazodone, nefazodone; imipramine; phenelzine; prazosin for nightmares associated with PTSD(64,66).
Regarding the ARS therapy, trauma-focused cognitive-behavioral psychotherapy is the first‑line choice and it may reduce the PTSD risk(65). The psychopharmacological interventions may also contribute to decreasing the risk of PTSD onset, for example by modulating plasma levels of glucocorticoids(67).
Substance-related disorders
The triad suicidal behavior – alcoholism – depression is an important clinical phenomenon in the general population, but it has also been reported in physicians(68-71). Self-medication with anxiolytics, sedatives and hypnotics in order to cope with occupational stress can lead to abuse and addiction(72). According to data from an epidemiological study in the UK, which involved 417 doctors, 44% had episodes of compulsive alcohol consumption and 5% met the criteria for alcohol dependence(73).
A study in healthcare professionals that assessed the risk factors for relapse (defined as the resuming the substance use after an initial diagnosis and a treatment program for chemical dependence was completed) revealed that 25% had at least one relapse(74). The self-administration of a potent opioid significantly increased the risk of relapse in the presence of coexisting mental disorders, but not in the absence of them(74). A family history of substance use disorder has been a strong predictor of relapse, and relapse was associated with an increased risk of subsequent relapses(74).
Doctors report substance abuse rates (including alcohol) ranging from 10% to 15%, compared to 9% in the general population, which were also correlated with an increased risk of suicide by intoxication(33,74). Alcohol, opioids and benzodiazepines are the most commonly abused substances in this population(75). The most often involved specialties in substance abuse are emergency medicine and anesthesia-intensive care(74-77). When substance dependence is detected in healthcare professionals, this pathology is usually in an advanced stage, compared to the general population(77). To this latency contribute the desire of people to maintain their professional status and various defenses such as rationalization or denial, which lead to the destruction of social, family and personal life long before the diagnosis of substance abuse or addiction is officially established(77,78).
The initial assessment is very difficult in this specific population, and it is recommended to recruit an experienced multidisciplinary team for diagnostic purposes(77-80). Individual and group psychotherapy, addiction-related psychoeducation, focusing the therapeutic approach on obtaining and maintaining the complete abstinence based on the 12-step method, are the most recommended therapeutic options for this population(77-79). Recognition of one’s maladaptive behaviors is facilitated by group therapy in which other doctors with addictive pathology are encouraged to participate, as well as the ventilation of emotions related to professional aspects (guilt, shame, fear etc.), which can be triggers for substance abuse(77,78).
The recovery rates in physicians who have been diagnosed with alcohol dependence are good, if they comply with the participation in therapy programs, with some longitudinal studies reporting values of 73% for remission over 17 years(81).
Conclusions
Occupational stress is a constant challenge for physicians and supportive staff, and the current context dominated by the COVID-19 pandemic leads to an exacerbation of work-related stress in the frontline professionals. The impact of these stressors over each medical professional is variable, but based on the analysis of data from the literature and data from other critical epidemiological situations (SARS-CoV, MERS-CoV, H1N1), it can be concluded that the risk of stress-related disorders is high in this specific population.
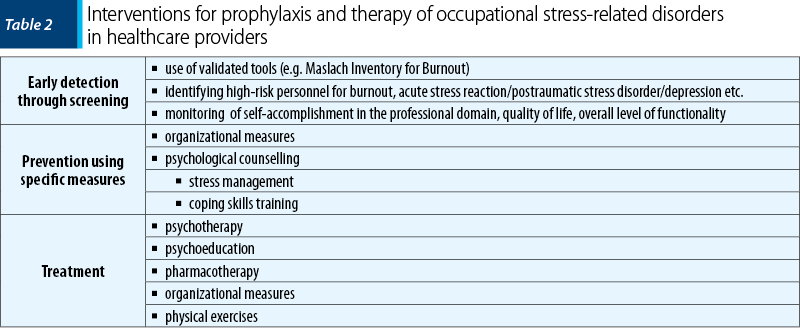
Based upon the data presented, it becomes obvious that there is a need to develop health policies for the prevention, early detection and treatment of stress-related disorders, in order to maintain the functional capacity and the health of frontline professionals, who are in the first line of the fight against the new type of coronavirus. Thus, stimulating the use of organizational tools (elaboration of an appropriate schedule, adequate distribution of responsibilities, with involvement in the decision-making act of the therapeutic team members, financial support for those who are needed to work overtime) and information on the available resources – psychologic and psychiatric care services, education on symptoms suggestive of burnout syndrome, acute stress reaction, major depression –, all these should be priorities for the institutions responsible for ensuring the quality of care during this difficult period.
Bibliografie
- Riviere M, Toullic Y, Lerouge P, et al. Management of work-related common mental disorders in general practice: a cross-sectional study. BMC Fam Pract. 2020;21:132.
- Ho CS, Chee CY, Ho RC. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann Acad Med Singap. 2020;49(1):1.
- WHO. Mental health and COVID-19. Accesat la adresa https://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/technical-guidance/mental-health-and-covid-19 în data de 27.08.2020.
- Spoorthy MS, Pratapa SK, Mahant S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic – A review. Asian J Psychiatr. 2020;51:102119.
- El-Hage W, Hingray C, Lemogne C, et al. Health professionals facing the coronavirus disease 2019 (COVID-19) pandemic: What are the mental health risks? Encephale. 2020;46(3S):S73-S80.
- Depression: What is burnout? InformedHealth.com, 2020. Available at: https://www.ncbi.nlm.nih.gov/books/NBK279286/ în data de 05.08.2020.
- Maslach C. Job stress and burnout. In: Paine, WS (Ed.). Understanding burnout: definitional issues in analyzing a complex phenomenon. Berverly Hills, CA, 1982.
- Wiederhold BK, Cipresso P, Pizzioli D, et al. Intervention for physician burnout: A systematic review. Open Med (Wars). 2018;13:253-263.
- Rotenstein LS, Torre M, Ramos MA, et al. Prevalence of burnout among physicians. A systematic review. JAMA. 2018;320(11):1131-1150.
- Vahey DC, Aiken LH, Sloane DM, et al. Nurse burnout and patient satisfaction. Med Care. 2004;42(Suppl.2):II57-II66.
- Rupert PA, Miller AO, Dorociak KE. Preventing burn-out: What does the research tell us? Research and Practice. 2015;46(3):168-174.
- Hakanen JJ, Schaufeli WB. Do burnout and work engagement predict depressive symptoms and life satisfaction? A three-wave seven-year prospective study. J Affect Disord. 2012;141(2-3):415-24.
- Salvagioni DAJ, Melanda FN, Mesas AE, et al. Physical, psychological and occupational consequences of job burnout: A systematic review of prospective studies. PLoS One. 2017;12(10):e0185781.
- Wurm W, Vogel K, Holl A, et al. Depression-burnout overlap in physicians. PLoS One. 2016;11(3):e0149913.
- OMS. ICD-10: Clasificarea internaţională a tulburărilor mentale şi de comportament. Ed. Trei, 2016.
- WHO. Burnout an “occupational phenomenon”: International Classification of Diseases. Accesat la adresa https://www.who.int/mental_health/evidence/burn-out/en/ în data de 05.08.2020.
- Maslach C, Jackson SE, Leiter MP. Maslach Burnout Inventory Manual, 3rd ed. Consult Psychol Press, Palo Alto, CA, 1996.
- Korczak D, Wastian M, Schneider M. Therapy of the burnout syndrome. GMS Health Technol Assess. 2012;8:Doc05.
- Maslach C, Goldberg J. Prevention of burnout: new perspectives. App Prevent Psychol. 1998;7:63-74.
- Maslach C, Leiter MP. Understanding the burnout experience: recent research and its implications for psychiatry. World Psychiatry. 2016;15(2):103-111.
- Aryankhesal A, Mohammadibakhsh R, Hamidi Y, et al. Interventions on reducing burnout in physicians and nurses: A systematic review. Med J Islam Repub Iran. 2019;33:77.
- Forcier K, Stroud LR, Papandonatos GD, et al. Links between physical fitness and cardiovascular reactivity and recovery to psychological stressors: A meta-analysis. Health Psychology. 2006;25(6):723-739.
- Salmon P. Effects of physical exercise on anxiety, depression and sensitivity to stress- a unifying theory. Clinical Psychology Review. 2001;21(1):33-61.
- Ochentel O, Humphrey C, Pfeifer K. Efficacy of exercise therapy in persons with burnout. A systematic review and meta-analysis. J Sports Sci Med. 2018;17(3):475-484.
- Dyrbye LN, Thomas MR, Massie FS, et al. Burnout and suicidal ideation among US medical students. Annals Int Med. 2008;149(5):334-341.
- Awa LW, Plaumann M, Walter U. Burnout prevention: A review of intervention programs. Patient Ed and Counseling. 2010;78(2):184-190.
- Deighton RM, Gurris N, Traue H. Factors affecting burnout and compassion fatigue in psychotherapists treating torture survivors: is the therapist’s attitude eto working through trauma relevant? J Trauma Stress. 2007;20:63-75.
- Dal Pai D, Lautert L, Souza SBC, et al. Violence, burnout and minor psychiatric disorders in hospital work. Rev Esc Enferm USP. 2015;49:457-64.
- Schramm E, Berger M. Interpersonal therapy for work-related stress depressive disorders. Nervenarzt. 2013;84(7):813-22.
- Blackmore ER, Stansfeld SA, Weller I, et al. Major depressive episodes and work stress: results from a national population survey. Am J Public Health. 2007;97(11):2088-2093.
- Bernburg M, Vitzthum K, Groneberg DA, Mache S. Physicians’ occupational stress, depressive symptoms and work ability in relation to their working environment: a cross-sectional study of differences among medical residents with various specialties working in German hospitals. BMJ Open. 2016;6(6):e011369.
- Koutsimani P, Montgomery A, Georganta K. The relationship between burnout, depression, and anxiety: A systematic review and meta-analysis. Front Psychol. 2019;10:284.
- Stanciu CN, Gnanasegaram SA, Brooks N III, et al. Physician wellness and substance use- a brief review. J Alcohol Drug Depend. 2018;6(3):1000e142.
- Mata DA, Ramos MA, Bansal N, et al. Prevalence of depression and depressive symptoms among resident physicians – A systematic review and meta-analysis. JAMA. 2015;314(22):2373-2383.
- Rout U, Cooper CL, Rout JK. Job stress among British general practitioners: predictors of job dissatisfaction and mental ill-health. Stress Med. 1996;12(3):155-166.
- Cooper GL, Clarke S, Rowbottom AM. Occupational stress, job satisfaction and well-being in anaesthetists. Stress Med. 2000;15(2):115-26.
- Cooper CL, Cartwright S. An intervention strategy for workplace stress. J Psychosom Res. 1997;43(1):7-16.
- Tennant C. Work-related stress and depressive disorders. J Psychosom Res. 2001;51:697-704.
- Mangalagiu AG, Riga S, Vasiliu O, Petrescu BM. Stress and pathogenesis of major depressive disorder. A narrative review. International Journal of Medical Dentistry. 2021;25(1):24-35.
- Sandahl C, Lundberg U, Lindgren A, et al. Two forms of group therapy and individual treatment of work-related depression: a one-year follow-up study. Int J Group Psychother. 2011;61:538-55.
- de Vibe M, Solhaug I, Rosenvinge JH, et al. Six-year positive effects of a mindfulness-based intervention on mindfulness, coping and well-being in medical and psychology students; results from a randomized controlled trial. PLoS One. 2018;13(4):e0196053.
- Neto JD, Myung E, Murta G, et al. Depression in the workplace: screening and treatment. Rev Assoc Med Bras. 2019;65(3):295-315.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 3rd ed., APA, Washington, 1980.
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed., Arlington, VA, APA, 2013.
- WHO. ICD-11. Available at: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/264310751 în data de 27.08.2020.
- Greenberg WM, Rosenfeld DN, Ortega EA. Adjustment disorder as an admission diagnosis. Am J Psychiatry. 1995;152(3):459-61.
- Strain JJ. The adjustment disorder diagnosis, its importance to liaison psychiatry, and its psychobiology. Int J Environ Res Public Health. 2019;16(23):4645.
- Nakamura J. Early detection and intervention for adjustment disorder and depression in the work place. Sishin Shinkeigaku Zasshi. 2012;114:1093-9.
- Polyakova I, Knobler HY, Ambrumova A, et al. Characteristics of suicidal attempts in major depression versus adjustment reactions. J Affect Disord. 1998;47:159-67.
- Nieuwenhuijsen K, Verbeek JHAM, Siemerink JCJM, Tummers-Nijsen D. Quality of rehabilitation among workers with adjustment disorders according to practice guidelines; a retrospective cohort study. Occup Environ Med. 2003;60(Suppl.II):i21-i25.
- Chirico F. Adjustment disorder as an occupational disease: Our experice in Italy. Occup Environ Med. 2016;7:52-57.
- Carta MG, Balestrieri M, Murru A, Hardoy MC. Adjustment disorder: epidemiology, diagnosis and treatment. Clin Pract Epidemiol Ment Health. 2009;5:15.
- O’Donnell ML, Metcalf O, Watson L, et al. A systematic review of psychological and pharmacological treatments for adjustment disorder in adults. J Trauma Stress. 2018;31:321-331.
- Quero S, Moles M, Campos D, et al. An adaptive virtual reality system for the treatment of adjustment disorder and complicated grief: 1-year follow-up efficacy data. Clin Psychol Psychother. 2019;26:204-217.
- Lazarus A. Traumatized by practice: PTSD in physicians. J Med Pract Manage. 2014;30(2):131-4.
- Lo T, De Stefano L, Lu S, et al. Post-traumatic stress disorder in resident physicians. Cureus. 2019;11(6):e4816.
- Somville FJ, De Gucht V, Maes S. The impact of occupational hazards and traumatic events among Belgian emergency physicians. Scand J of Trauma, Resusc and Em Med. 2016;24:59.
- Atwoli L, Stein DJ, Williams DR, et al. Trauma and posttraumatic stress disorder in South Africa: Analysis from the South African stress and health study. BMC Psychiatr. 2013;13:182.
- Einav S, Shalev AY, Ofek H, et al. Differences in psychological effects in hospital doctors with and without post-traumatic stress disorder. Br J Psychiatry. 2008;193(2):165-6.
- Walton M, Murray E, Christian MD. Mental health care for medical staff and affiliated healthcare workers during the COVID-19 pandemic. Eur Heart J Acute Cardiovasc Care. 2020;2048872620922795.
- Vyas KJ, Delaney EM, Jennifer A, et al. Psychological impact of deploying in support of the US response to Ebola: a systematic review and meta-analysis of past outbreaks. Mil Med. 2016;181(11):1515-31.
- Xiao S, Luo D, Xiao Y. Survivors of COVID-19 are at high risk of posttraumatic stress disorder. Glob Health Res Policy. 2020;5:29.
- Watkins LE, Sprang KR, Rothbaum BO. Treating PTSD: A review of evidence-based psychotherapy interventions. Front Behav Neurosci. 2018;12:258.
- Charney ME, Hellberg SN, Bui E, Simon NM. Evidence-based treatment of posttraumatic stress disorder: An updated review of validated psychotherapeutic and pharmacological approaches. Harv Rev Psychiatry. 2018;26(3):99-115.
- Vasiliu O, Vasile D, Mangalagiu AG, et al. Current treatment of posttraumatic stress disorder – A review of therapeutic guidelines and good practice recommendations. Romanian Journal of Military Medicine. 2020;CXXIII(4):241-248.
- Lancaster CL, Teeters JB, Gros DF, Back SE. Posttraumatic stress disorder: Overview of evidence-based assessment and treatment. J Clin Med. 2016;5(11):105.
- Bryant RA. The current evidence for acute stress disorder. Curr Psychiatr Rep. 2018;20(12):111.
- Tyssen R. Work and mental health in doctors: A short review of Norwegian studies. Porto Biomed J. 2019;4(5):e50.
- Tyssen R. Mental health problems among medical students and young physicians. A nationwide and longitudinal study. Department of Behavioural Sciences in Medicine, Univ of Oslo, 2001.
- Vasiliu O, Vasile D, Vasiliu DG, Ciobanu OM. Quality of life impairments and stress coping strategies during the COVID-19 pandemic isolation and quarantine – A Web-based survey. Romanian Journal of Military Medicine. 2021;CXXIV(1):10-21.
- Vasiliu O, Vasile D. Cultural and hystorical aspects of the psychoactive drugs consumption. Romanian Journal of Military Medicine. 2011;2(CXIV):33-39
- Rosvold EO, Tyssen R. Should physicians’ self-prescribing be restricted by law? Lancet. 2005;365:1372-74.
- Medisauskaite A, Kamau C. Does occupational distress raise the risk of alcohol use, binge-eating, ill health and sleep problems among medical doctors? A UK cross-sectional study. BMJ Open. 2019;9:e027362.
- Hughes PH, Brandenburg N, Baldwin DC, et al. Prevalence of substance use among US physicians. JAMA.1992;267:2333-2339.
- Domino KB, Hornbein TF, Polissar NL, et al. Risk factors for relapse in health care professionals with substance use disorders. JAMA. 2005;293(12):1453-60.
- Merlo LJ, Gold MS. Prescription opioid abuse and dependence among physicians: hypotheses and treatment. Harv Rev Psychiatry. 2008;16:181-194.
- Gourlay DL, Heit HA. Pain and addiction: managing risk through comprehensive care. J Addict Dis. 2008;27:23-30.
- Berge KH, Seppala MD, Schipper AM. Chemical dependency and the physician. Mayo Clin Proc. 2009;84(7):625-631.
- Talbott GD, Gallegos KV, Wilson PO, Porter TL. The Medical Association of Georgia’s Impaired Physicians program. Review of the first 1000 physicians: analysis of specialty. JAMA. 1987;257(21):2927-2930.
- Graham AW, Schultz TK, Mayo-Smith MF, et al. principles of Addiction Medicine, 3rd ed., Chevy Chase Ed., American Society of Addiction Medicine, 2007.
- Lloyd G. One hundred alcoholic doctors: A 21-year follow-up. Alcohol and Alcoholism. 2002;37(4):370-374.
Articole din ediţiile anterioare
„Adolescenţa complicată” – între agresivitate şi depresie
Cu toate că în multe situaţii dau impresia unui adult mai tânăr, adolescenţii prezintă un tablou clinic al patologiilor psihiatrice diferit de cel ...
Comorbidităţile asociate depresiei
Depresia este una dintre cauzele care duc la declin în funcţionarea socioprofesională şi la scăderea calităţii vieţii. De multe ori, depresia este ...
Importanţa reintegrării sociale în cazul pacienţilor cu tulburare depresivă majoră
Tulburarea depresivă majoră este principala cauză a dizabilităţii la nivel mondial, aceasta fiind asociată cu tulburări de consum de substanţe, num...
Integrarea datelor farmacogenetice în practica psihiatrică
Medicina personalizată este un deziderat care prezintă avantajele unei eficacităţi sporite şi ale unei tolerabilităţi superioare, aspecte care ar î...