Introduction. Suicide is a global public health concern, with a significant impact on mortality rates. This study explores the complex interplay between spirituality, resilience and the suicide risk in Romanian patients diagnosed with depression.
Materials and method. A clinical sample of 65 depressed inpatients participated in this study. Demographics, suicide risk, spirituality and resilience were assessed using standardized instruments. Statistical analyses were performed to identify correlations between suicide risk, resilience and spirituality.
Results. The study reveals a significant negative correlation between spirituality and suicide risk, as well as between resilience and suicide risk among depressed patients. Those with higher levels of spirituality and resilience exhibited a reduced suicide risk.
Discussion. This study emphasizes the critical role of depressive symptoms as predictors of suicidal behavior in individuals with mood disorders. It also highlights the protective influence of spirituality and resilience, suggesting that interventions focused on enhancing these aspects could improve the mental well-being of depressed patients and reduce the suicide risk. The findings underscore the need for comprehensive, holistic approaches to mental healthcare.
Conclusions. Targeted interventions that incorporate spirituality and resilience may enhance the quality of life for depressed patients and contribute to suicide prevention efforts. Future research should explore intervention strategies that harness spirituality to strengthen resilience in diverse populations. While this study provides valuable insights, prospective research is essential to establish causal relationships, and multicenter studies should include more diverse participant populations.
The influence of spirituality and resilience on suicide risk in Romanian patients with depression
Influenţa spiritualităţii şi a rezilienţei asupra riscului suicidar la pacienţii depresivi din România
First published: 29 septembrie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Psih.74.3.2023.8692
Abstract
Rezumat
Introducere. Suicidul este o preocupare globală majoră în domeniul sănătăţii publice, cu un impact semnificativ asupra ratei mortalităţii. Acest studiu explorează interacţiunea complexă dintre spiritualitate, rezilienţă şi riscul suicidar în rândul pacienţilor români diagnosticaţi cu depresie.
Materiale şi metodă. Un eşantion clinic format din 65 de pacienţi internaţi cu depresie a fost inclus în acest studiu. Au fost evaluate datele demografice, riscul suicidar, spiritualitatea şi rezilienţa, utilizând instrumente standardizate. Analizele statistice au fost efectuate pentru a identifica corelaţiile dintre riscul suicidar, rezilienţă şi spiritualitate.
Rezultate. Studiul relevă o corelaţie semnificativă negativă între spiritualitate şi riscul suicidar, precum şi între rezilienţă şi riscul suicidar, în rândul pacienţilor cu depresie. Cei cu niveluri mai ridicate de spiritualitate şi rezilienţă au prezentat un risc mai scăzut de suicid.
Discuţie. Acest studiu subliniază rolul critic al simptomelor depresive ca predictor al comportamentului suicidar în rândul persoanelor cu tulburări de dispoziţie. De asemenea, evidenţiază influenţa protectoare a spiritualităţii şi rezilienţei, sugerând că intervenţiile axate pe consolidarea acestor aspecte ar putea îmbunătăţi starea mintală a pacienţilor cu depresie şi ar putea reduce riscul suicidar. Rezultatele subliniază necesitatea unor abordări comprehensive şi holistice în îngrijirea sănătăţii mintale.
Concluzii. Intervenţiile direcţionate care includ spiritualitatea şi rezilienţa pot îmbunătăţi calitatea vieţii pacienţilor cu depresie şi pot contribui la eforturile de prevenire a suicidului. Cercetările viitoare ar trebui să exploreze strategii de intervenţie care să valorifice spiritualitatea pentru a consolida rezilienţa în populaţii diverse. Cu toate că acest studiu oferă perspective valoroase, cercetarea prospectivă este esenţială pentru a stabili relaţii cauzale, iar studiile multicentrice ar trebui să includă populaţii de participanţi mai diversificate.
Introduction
Suicide is a globally widespread phenomenon, with approximately 700,000 people dying from suicide each year. According to World Health Organization (WHO), suicide was the 17th most common cause of mortality in 2015. In Romania, the mortality rate due to suicide is 11.7 per 100,000 inhabitants(1).
Numerous research endeavors have delved into the diverse facets of spirituality and resilience, seeking a deeper comprehension of the link between spirituality/religiosity, resilience, and the risk of suicide. The question that lingers pertains to whether this connection varies among distinct religious communities. Spirituality encompasses a wide-ranging concept that finds definition in experiences tied to either the transcendent realm or connections with oneself, others, and the natural world(2). While spirituality can intertwine with religious beliefs and practices, it is not inherently linked to them. Religiosity, on the other hand, often manifests spirituality through various practices specific to a particular religious affiliation(3).
Research indicates that despair and depressive symptoms serve as robust predictors of suicidal behavior in individuals diagnosed with mood disorders(4,5). The role of spirituality in this context is significant, as it can foster a positive coping mechanism, instill hope, alleviate stress and provide solace(6,7).
Numerous studies have established a connection between spirituality and a reduced risk of suicide(6,8,9). One review study found that 84% of studies reported a lower prevalence of suicidal behavior among individuals who considered themselves more spiritual(10). Another review of the literature reported that religiosity has a favorable effect on the risk of suicide(11). Bonelli and Koenig’s literature review found that higher levels of spirituality/religiosity were inversely correlated with completed suicide(12).
Conversely, research suggests that maladaptive aspects of spirituality, such as negative religious coping and a limited capacity for forgiveness, can be linked to suicide risk(13).
Studies have shown that spirituality and resilience are intertwined. Resilience is a complex concept that can be defined as the capacity to cope and adapt when faced with adverse events (hardship, tragedy, trauma, life stressors)(14). It can be nurtured through a person’s religious beliefs, spirituality, supportive relationships and enhanced self-esteem. Spirituality plays a pivotal role in enhancing resilience, especially among older individuals(15,16). It bolsters an individual’s capacity to confront and adapt to challenging life events, ranging from illness and loss to warfare and natural disasters(17).
Several studies have explored the relationship between resilience and suicide, consistently demonstrating that resilience serves as a protective factor against the risk of suicide(18-20). For instance, a longitudinal study investigating the association between resilience and suicidal ideation and attempts found that a high level of resilience predicted a lower risk of suicide during follow-up assessments(21).
Methodology
This study sought to examine the influence of spirituality and resilience on suicide risk in a clinical sample of depressed patients.
Study design and participants
Sixty-five consecutive inpatients diagnosed with unipolar or bipolar depression, aged between 18 and 70 years old, were recruited from the Psychiatry Ward III of the Cluj-Napoca County Emergency Hospital. Data were collected between January and June 2022. The inclusion criteria encompassed a diagnosis of depression (depressive episode – F32; recurrent depressive disorder – F33) following ICD-10 criteria.
The exclusion criteria included participants over 70 years old and those with other psychiatric disorders (such as schizophrenia, delirium, delusional disorder, mental retardation, cognitive impairment or substance use disorder) or neurological disorders.
Ethical considerations
The study received approval from the university Ethics Committee. Researchers provided participants with detailed information about the research, emphasizing its voluntary and confidential nature and their right to withdraw at any point. The participants were assured that there were no associated risks. The written consent was obtained from all participants.
Measures
The participants completed a demographic questionnaire gathering sociodemographic information, including gender, age, marital status, residence, religious affiliation and educational background.
Columbia Suicide Severity Rating Scale (C-SSRS)
Developed by Kelly Posner and collaborators, this scale assesses and classifies the suicide risk. It comprises 17 items that evaluate four dimensions: suicidal ideation, intensity of ideation, suicidal behavior, and actual suicide attempts. The C-SSRS is also a reliable screening instrument known for its validity, sensitivity/specificity and internal consistency(22).
Connor-Davidson Resilience Scale (CD-RISC 25)
An assessment tool for resilience, CD-RISC 25 comprises 25 items rated on a five-point Likert scale (ranging from 0 to 4), with total scores ranging from 0 to 100. It measures an individual’s capacity to bounce back from adversity(23).
Daily Spiritual Experiences Scale (DSES)
Developed by Lynn Underwood, DSES assesses experiences of connection with the sacred or transcendent in everyday life. It has 16 items, the first 15 items being rated on a six-point Likert type scale, ranging from 1 (“many times a day”) to 6 (“never or almost never”). Item 16 has responses ranging from 1 (“as close as possible”) to 4 (“not at all”)(24). The first 15 items were used in this study, with reverse coding applied, meaning higher scores indicate a higher frequency of spiritual experiences.
Data analysis
All analyses were performed using Statistical Package for the Social Sciences (SPSS) software, version 26, for Windows. The descriptive analysis was used to characterize the sample. Quantitative variables were expressed as mean ± standard deviation (SD), and qualitative variables were expressed as frequency and percentage values. We used linear regression to determine Pearson coefficient.
Results
The group included in this study exhibited a diverse range of sociodemographic characteristics (Table 1). Ages ranged from 19 to 69 years old, representing a broad age spectrum. The gender distribution showed an almost equitable split, with a little over half of the participants being women (53.1%). Additionally, the study encompassed individuals from various geographical backgrounds, with 53.1% originating from urban areas.
Regarding religious affiliation, the predominant faith among participants was Orthodox Christianity, accounting for 78.1% of the sample. Marriage status was another noteworthy aspect, with a significant majority of participants being married, constituting 68.8% of the total. Furthermore, in terms of educational attainment, a substantial proportion of patients had completed only secondary studies, amounting to 48.4% of the cohort.
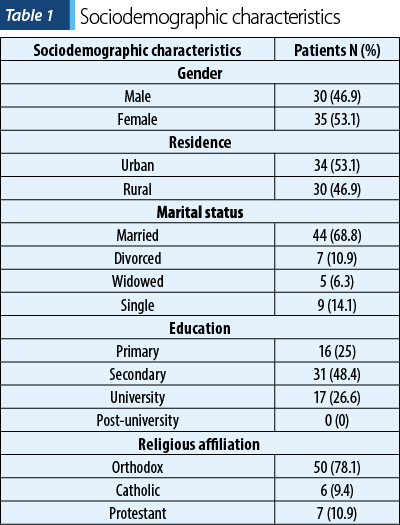
Table 2 displays the means and standard deviations of the DSES scores, the CD-RISC 25 scores, and the score of CSSR suicidal ideation severity subscale. In order to determine the relationship between spirituality, resilience and suicide risk, we calculated the Pearson correlation coefficient.
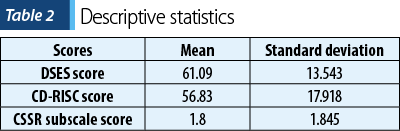
Table 3 presents the results of simple linear regression conducted between the CSSR scores and the CD-RISC 25 scores. The linear regression identified a weak negative correlation (Pearson coefficient = -0.298) between the severity of suicidal ideation and the level of resilience (measured by the CD-RISC 25 score) at an alpha value of 0.01 (p<0.05).
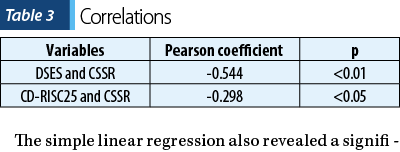
The simple linear regression also revealed a significant negative correlation (Pearson coefficient = -0.544) between the severity of suicidal ideation (measured by the CSSR score) and the level of spirituality (DSES score), at p<0.01.
Discussion
Suicide remains a pressing global concern, with a substantial number of lives lost each year. Our study focused on the specific context of Romania, where suicide has been a significant cause of mortality. This context underscores the urgency of exploring factors that may contribute to suicide risk. Our investigation delved into the complex interplay between spirituality, resilience, and the risk of suicide among depressed patients.
Our study acknowledged the multifaceted nature of spirituality, which can manifest in various forms, including connections with the transcendent, self, others and nature. It’s important to note that spirituality is not synonymous with religiosity, although they can intersect. Religiosity often involves specific forms of manifestation.
Our findings align with prior research, highlighting the significance of depressive symptoms and despair as robust predictors of suicidal behavior among individuals grappling with mood disorders. This observation underscores the gravity of addressing the mental health challenges faced by this population.
We found substantial evidence linking spirituality to a reduced risk of suicide. This correlation suggests that spirituality can serve as a protective factor, fostering positive coping mechanisms, nurturing hope, mitigating stress, and offering solace to individuals facing emotional distress. The study we conducted consistently pointed to lower suicide prevalence among those who identified as more spiritual, reinforcing the potential role of spirituality in enhancing mental well-being.
Our study also examined the concept of resilience, defined as the capacity to adapt and cope effectively in the face of adversity. Our investigation, consistent with existing research, demonstrated that resilience acts as a protective factor against the risk of suicide. This finding underscores the importance of cultivating resilience in individuals at risk of suicidal behavior. It implies that interventions aimed at enhancing resilience, particularly among those with depression, may contribute to suicide prevention efforts.
The findings of our study hold practical implications for mental health practitioners and policymakers. Recognizing the potential protective effects of spirituality and resilience, interventions can be tailored to incorporate these elements into treatment strategies for individuals at risk of suicide. This might involve fostering spiritual support networks, encouraging practices that enhance resilience, and considering the spiritual and existential dimensions of therapy.
The holistic approach adopted in this study, encompassing spiritual and psychological dimensions, underscores the importance of addressing mental health from a comprehensive perspective. It acknowledges that individuals are not merely defined by their symptoms but also by their spiritual and existential beliefs, which can significantly influence their coping mechanisms and the overall well-being.
While our study offers valuable insights, it has limitations. Its observational, cross-sectional design restricts the ability to establish causal relationships between spirituality, depression and the suicide risk. Prospective studies are essential for elucidating these connections further.
Additionally, the study’s sample predominantly comprised individuals from the Christian Orthodox tradition, reflecting Romania’s religious demographics. Therefore, our findings may not be readily generalizable to populations with different religious affiliations. Future research should adopt a multicenter approach, encompassing larger and more diverse patient populations, from various countries and religious backgrounds.
Conclusions
Our study underscores the importance of targeted interventions aimed at enhancing the psychological well-being of depressed patients. Implementing strategies that bolster resilience and spirituality could prove instrumental in elevating their overall quality of life and mitigating the challenges associated with depression and suicide behavior. Subsequent research endeavors might explore potential interventions that seamlessly integrate spirituality as a conduit to fortify resilience, ultimately leading to improved health outcomes in patients diagnosed with depression. Developing tailored programs geared towards enhancing resilience holds promise in guiding patients towards more favorable life adjustments while grappling with their illness.
In summary, our study sheds light on the intricate relationship between spirituality, resilience and the suicide risk among depressed patients. It highlights the potential protective role of spirituality and resilience in mitigating suicide risk, emphasizing the importance of considering these factors in mental health interventions and suicide prevention strategies. However, further research is needed to deepen our understanding of these connections and their applicability to diverse populations.
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
-
WHO. Suicide data. WHO [Internet]. 2017 [cited 2017 Dec 10]. http://www.who.int/mental_health/prevention/suicide/suicideprevent/en/#
-
Meraviglia MG. Critical analysis of spirituality and its empirical indicators. Prayer and meaning in life. J Holist Nurs. 1999;17(1):18-33.
-
Campesino M, Schwartz GE. Spirituality among Latinas/os: implications of culture in conceptualization and measurement. ANS Advances Nursing Science. 2006;29(1):69–81.
-
Britton PC, Duberstein PR, Conner KR, Heisel MJ, Hirsch JK, Conwell Y. Reasons for living, hopelessness, and suicide ideation among depressed adults 50 years or older. Am J Geriatr Psychiatry. 2008;16(9):736-741.
-
Chioqueta AP, Stiles TC. Personality traits and the development of depression, hopelessness, and suicide ideation. Personality and Individual Differences. 2005;38(6):1283–1291.
-
Abdollahi A, Abu Talib M. Hardiness, spirituality, and suicidal ideation among individuals with substance abuse: the moderating role of gender and marital status. J Dual Diagn. 2015;11(1):12-21.
-
Cotton S, Kudel I, Roberts YH, et al. Spiritual well-being and mental health outcomes in adolescents with or without inflammatory bowel disease. J Adolesc Health. 2009;44(5):485-492.
-
Garroutte EM, Goldberg J, Beals J, Herrell R, Manson SM; AI-SUPERPFP Team. Spirituality and attempted suicide among American Indians. Soc Sci Med. 2003;56(7):1571-1579.
-
McClain-Jacobson C, Rosenfeld B, Kosinski A, Pessin H, Cimino JE, Breitbart W. Belief in an afterlife, spiritual well-being and end-of-life despair in patients with advanced cancer. Gen Hosp Psychiatry. 2004;26(6):484-486.
-
Koenig HG. Religion, spirituality, and health: the research and clinical implications. ISRN Psychiatry. 2012;2012:278730.
-
Zagozdzon P. Zwiqzek miedzy religia a zdrowiem w badaniach epidemiologicznych [Religiosity and health in epidemiological studies]. Pol Merkur Lekarski. 2012;32(191):349-353.
-
Bonelli RM, Koenig HG. Mental disorders, religion and spirituality 1990 to 2010: a systematic evidence-based review. J Relig Health. 2013;52(2):657-673.
-
Kopacz MS, Currier JM, Drescher KD, Pigeon WR. Suicidal behavior and spiritual functioning in a sample of Veterans diagnosed with PTSD. J Inj Violence Res. 2016;8(1):6-14.
-
Wu G, Feder A, Cohen H, Kim J, Calderon S, Charney D, Mathé A. Understanding resilience. Frontiers in Behavioral Neuroscience. 2013;7:1–15.
-
Manning LK. Navigating hardships in old age: Exploring the relationship between spirituality and resilience in later life. Qualitative Health Research. 2013;23:568–575.
-
Vahia I, Depp C, Palmer B, Fellows I, Golshan S, Thompson W, et al. Correlates of spirituality in older women. Aging & Mental Health. 2011;15(1):97–102.
-
Ramsey JL. Spirituality and aging: Cognitive, affective, and relational pathways to resiliency. Annual Review of Gerontology and Geriatrics, 2012;32(1):131-150.
-
Liu DW, Fairweather-Schmidt AK, Roberts RM, Burns R, Anstey KJ. Does resilience predict suicidality? A lifespan analysis. Arch Suicide Res. 2014;18(4):453–464.
-
Roy A, Sarchiapone M, Carli V. Low resilience in suicide attempters. Arch Suicide Res. 2007;11(3):265–269.
-
Matel-Anderson DM, Bekhet AK, Garnier-Villarreal M. Mediating effects of positive thinking and social support on suicide resilience. West J Nurs Res. 2019;41(1):25–41.
-
Youssef NA, Green KT, Beckham JC, Elbogen EB. A 3-year longitudinal study examining the effect of resilience on suicidality in veterans. Ann Clin Psychiatry. 2013;25(1):59–66.
-
Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168(12):1266-1277.
-
Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76-82.
-
Underwood LG, Teresi JA. The daily spiritual experience scale: development, theoretical description, reliability, exploratory factor analysis, and preliminary construct validity using health-related data. Ann Behav Med. 2002;24(1):22-33.
Articole din ediţiile anterioare
EPA Statement for The World Mental Health Day Working together to prevent suicide
10th of October 2019 – On the occasion of today’s World Mental Health Day, in addition to the key messages delivered on 10th of September, the Euro...
Psychopathological and contextual factors of suicide in alcoholism
Forty percent of people with alcohol-related disorders checking into rehabilitation profile clinics admit at least one suicide attempt(1). The suic...
Sleep and depression – understanding the bidirectional relationship
Sleep and depression are two interconnected conditions that have a bidirectional relationship. On one hand, depression can lead to sleep problems, ...
Mental health and self-esteem correlated with the academic achievements of youths from Sri Lankan schools
Every human being experiences different phases of life in which the youth period is crucial, valuable and productive. It is also a settling down ag...