Background and aim. The worldwide rise of caesarean section (CS) is a major public health concern and a cause of significant debate due to potential maternal and perinatal risks, cost issues and inequity in access. In the Republic of Moldova, in recent years, the incidence of CS has increased by 7.7% (from 12.08% in 2007 to 20.5% in 2019); however, perinatal mortality rates haven’t changed (10.3‰ in 2007, and 9.7‰ in 2019). In order to understand the factors that determine the increasing trend of CS and to approach new strategies to reduce unnecessary caesarean sections, a standardized tool is needed to assess and compare CS rates. Methodology. A single-center, cross-section study was conducted in the period of January-December 2019. Data were collected from medical charts of women who gave birth in the Department of Obstetrics and Gynecology of the “Gheorghe Paladi” Municipal Clinical Hospital, Chişinău, and classified using the ten-group classification system according to Robson, to determine the CS rate in each group, the absolute and relative contribution made by each group to the overall caesarean section rate. Results. A total of 4279 deliveries were analyzed, and of these, 836 (19.5%) cases were delivered by caesarean section. The most representative group of our population was Group 3 (42.4%), followed by Group 1 (32.1%) and Group 5 (7.5%). The greatest contributors to the overall CS rate were Group 5 (33.8%), Group 2 (14.7%) and Group 1 (11.4%). There was also a high rate of pre-labor caesarean sections in Group 2, Group 4 and Group 10. Conclusions. The obtained results indicate that the greatest contributor to CS rate are women with previous caesarean section, followed by nulliparous women with full-term, cephalic pregnancy. An important step in reducing the total CS rate is to focus our efforts on decreasing the caesarean section rate in primary patients. We found that the Robson classification is clinically relevant and it is an effective tool for analyzing the caesarean section rate in our population.
Analiza ratei operaţiilor cezariene în conformitate cu sistemul de clasificare Robson, în cadrul Spitalului Clinic Municipal din Republica Moldova
Analysis of caesarean section rates according to Robson’s classification at the Municipal Clinical Hospital, Republic of Moldova
First published: 30 decembrie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.70.4.2022.7495
Abstract
Rezumat
Introducere şi scop. Creşterea globală a ratei operaţiei cezariene (OC) reprezintă un subiect major de preocupare şi dezbatere pentru sănătatea publică, din cauza riscurilor materne şi perinatale asociate, a problemelor financiare implicate şi a inechităţii privind accesul la asistenţă medicală calificată. În ultimul deceniu, în Republica Moldova, incidenţa naşterii prin OC a crescut cu 7,7% (de la 12,08% în 2007 la 20,5% în 2019). Cu toate acestea, rata mortalităţii perinatale nu s-a schimbat semnificativ, constituind 10,3‰ în 2007 şi 9,7‰ în 2019. Pentru a identifica factorii ce determină tendinţa de creştere a ratei OC, în scopul elaborării şi implementării noilor strategii de reducere a ratei operaţiilor cezariene, este absolut necesar un instrument standardizat de evaluare şi comparare a ratelor acestor operaţii. Metodologie. În perioada ianuarie-decembrie 2019, a fost efectuat un studiu transversal în care au fost incluse femeile care au născut în cadrul Departamentului de Obstetrică şi Ginecologie al Spitalului Clinic Municipal „Gheorghe Paladi”, Chişinău, şi au fost clasificate în conformitate cu Sistemul de clasificare în 10 grupuri propus de Robson. Pentru fiecare grup s-au calculat rata operaţiei cezariene şi contribuţia absolută şi relativă a OC. Rezultate. Au fost analizate 4279 de naşteri. Dintre acestea, 836 de femei (19,5%) au născut prin operaţie cezariană. Cel mai reprezentativ grup al populaţiei obstetricale îl reprezintă Grupul 3 (42,4%), urmat de Grupul 1 (32,1%) şi de Grupul 5 (7,5%). Cei mai mari contribuitori la rata totală a operaţiilor cezariene au fost Grupul 5 (33,8%), Grupul 2 (14,7%) şi Grupul 1 (11,4%). De asemenea, s-a înregistrat o rată mare a OC efectuate înainte de debutul travaliului în Grupul 2, Grupul 4 şi în Grupul 10. Concluzii. Prin implementarea clasificării Robson, am identificat că cele mai mari grupuri care contribuie la rata operaţiilor cezariene în cazul populaţiei noastre le reprezintă femeile cu cicatrice uterine după OC în anamneză, urmate de femeile nulipare cu sarcină unică în prezentaţie craniană, la termen. Un pas important în reducerea ratei operaţiilor cezariene îl reprezintă concentrarea eforturilor noastre pentru a reduce numărul operaţiilor cezariene inutile la femeile nulipare (Grupurile 1 şi 2). Clasificarea Robson este relevantă clinic şi reprezintă un instrument eficient de analiză a ratei operaţiilor cezariene.
Introduction
The worldwide rise of the caesarean section (CS) rate is a major topic of debate and a significant concern for global public health, particularly regarding its potential maternal and perinatal risks(1).
In order to identify the possible causes that determine the continuous increase of CS, to monitor and compare the caesarean section rates in a constant manner, it is necessary to implement a standardized, internationally accepted classification system(2). The designation and implementation of a single classification system allow the audit, analysis and comparison of CS rates in different medical institutions.
The World Health Organization (WHO) has proposed the Robson classification in ten groups, as a global standard tool for evaluating, monitoring and comparing CS rates in each medical institution and between them(2,3).
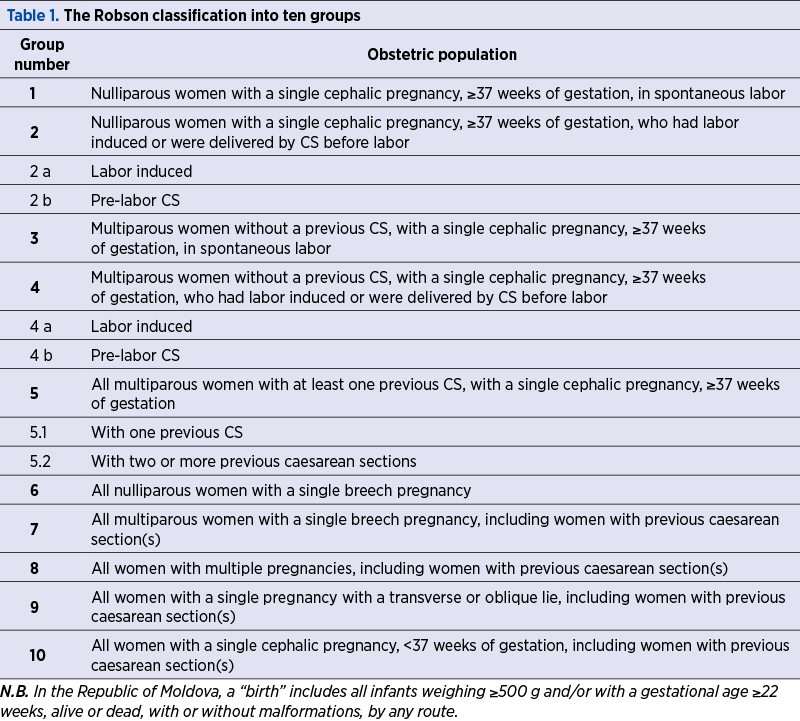
The Robson classification provides a critical analysis in conformity with pregnancy’s characteristics, being based on simple obstetrical parameters, such as parity, history of a previous caesarean section, gestational age, onset of labor, fetal presentation and lie, and the number of fetuses. The Robson classification system is firm about the fact that a woman’s pregnancy can only be classified into one group.
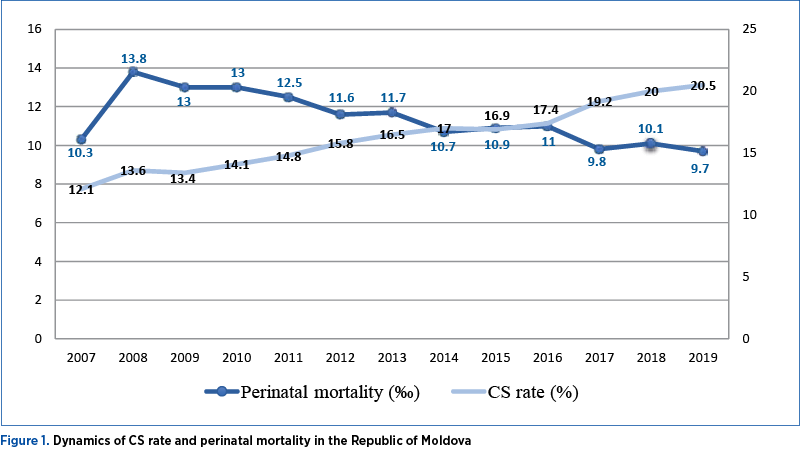
In the Republic of Moldova, the CS rate is in a continuing raising trend, from 12% in 2007 to 20.5% in 2019; however, the perinatal mortality hasn’t changed since 2007, constituting 10.3‰ and 9.7‰ in 2019 (Figure 1), this phenomenon requiring a good evaluation followed by the development and implementation of new strategies to reduce caesarean delivery.
The Society of Obstetricians and Gynecologists of the Republic of Moldova advocates the implementation of the Robson classification system recommended by the WHO as a global standard for recording and monitoring caesarean sections, in order to understand which are the factors that determine the increasing tendency of the number of deliveries by CS and to propose and implement strategies to avoid unnecessary surgeries(4).
The aim of this study was to analyze caesarean section by applying the Robson classification in ten groups, in order to identify the target groups of women that most of all influence the CS rate and to argue the necessity of implementation of this classification system in reducing the unnecessary caesarean sections.
Methodology
This is a cross-sectional study conducted within the Department of Obstetrics and Gynecology of the “Gheorghe Paladi” Municipal Clinical Hospital (MCH) in Chişinău, which is a secondary level medical institution. In the study, there were included women who gave birth between January and December 2019 in the hospital and were classified into Robson ten groups, according to Table 1, in order to calculate the CS rate in each group, the absolute and relative contribution of each group to the total caesarean sections rate(5).
The obtained data were analyzed according to WHO recommendations stipulated in the Robson classification manual(5) and summarized according to standardized tables.
According to the WHO methodology, the analysis follows several key steps.
First of all, each birth case was classified into one of the Robson groups (Table 1), using six basic variables (parity, previous CS, onset of labor, number of fetuses, gestational age, fetal presentation and lie).
Secondly, the data were assessed for quality, population type and CS rates.
Specifically, there were used the following types of variables collected from the patient database: maternal age, gestational age, maternal pathological conditions (such as diabetes, hypertensive disorders and others), fetal pathological conditions, indications for CS.
For each stage, the results were compared with reference data for interpretation according to Robson and the results of the WHO Multicountry Survey on Maternal and Newborn Health (WHO MCS)(6-8).
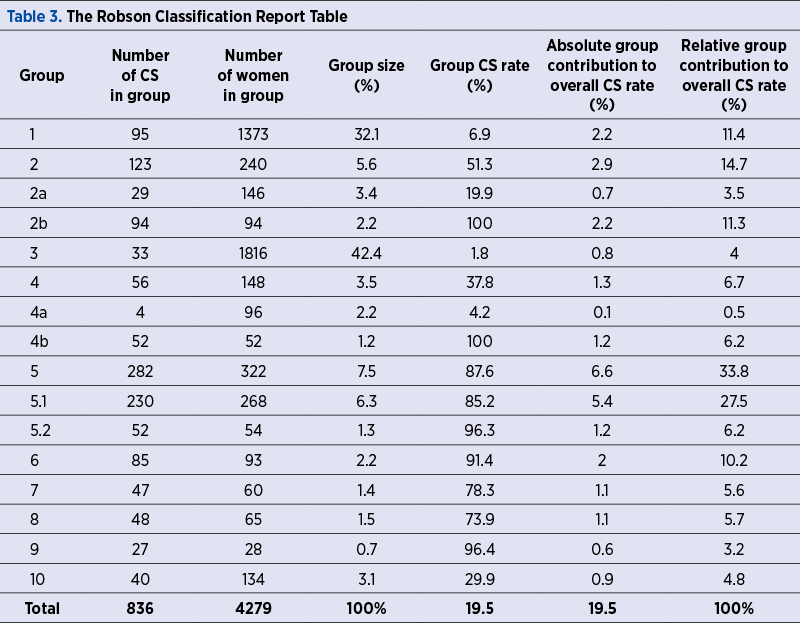
All analyzed variables were entered in the questionnaire within the Epi INFO program version 7.2.1.0. For each group, there were calculated: 1) Number of CS in the group; 2) Group size (%) which is calculated as a ration between the number of women in the group and total number of women delivered in the hospital x 100; 3) Group CS rate (%) = number of CS in the group/total number of women in the group x 100; 4) Absolute group contribution to overall CS rate (%) = number of CS in the group/total number of women delivered in the hospital x 100; and 4) The relative group contribution to overall CS rate (%) = number of CS in the group/total number of CS in the hospital x 100. All these data and percentages were presented in the Report Table of Robson Classification (Table 3).
Results
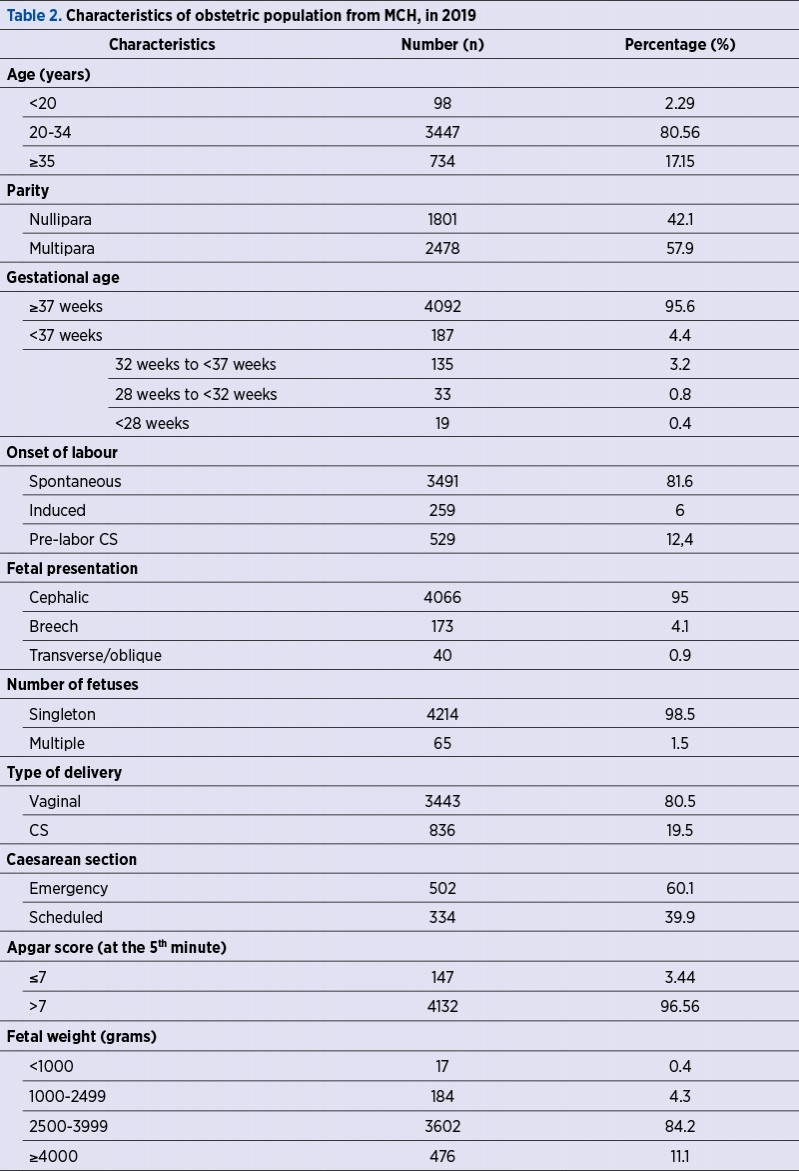
During the study, 4279 births were registered in the Department of Obstetrics and Gynecology of the MCH. The average age of women was 29.1 (±5.3) years old. Among them, 3443 women (80.5%) gave birth vaginally and 836 women (19.5%) delivered by caesarean section (Table 2), with about a third (39.9%) of all caesarean section performed before the onset of labor. Labor induction was recorded in 259 cases (6%).
Premature births (before 37 weeks) were recorded in 4.4% of cases, 0.4% of all newborns were extremely premature (less than 28 weeks), and 0.8% had severe prematurity (28 weeks to 32 weeks).
In order to identify and analyze the groups of women who contributed the most or the least to the overall CS rate, all women who gave birth during the reference period were classified into the ten Robson groups, shown in Table 3 (modified by adding the information about Groups 2a and 2b, 4a and 4b).
According to the data presented in Table 3 about the relative size of each group, we can see that Group 3 (multiparous women without a previous CS, with a single cephalic pregnancy, ≥37 weeks of gestation, in spontaneous labor) is the most representative group of our obstetrical population, representing 42.4%, followed by Group 1 (nulliparous women with a single cephalic pregnancy, ≥37 weeks of gestation, in spontaneous labor) which constituted 32.1%. Group 5 (all multiparous women with at least one previous caesarean section, with a single cephalic pregnancy, ≥37 weeks of gestation) was the third group in terms of size (7.5%), followed by Group 2 (nulliparous women with a single cephalic pregnancy, ≥37 weeks of gestation, who had labor induced or were delivered by caesarean section before labor), with 5.6%.
Analyzing the relative contribution of each group to the overall CS rate (the ration between the number of caesarean sections in the group and the total number of caesarean sections during the study period), we determined that the main contributor to the overall CS rate was Group 5 (all multiparous women with at least one previous caesarean section, with a single cephalic pregnancy, ≥37 weeks of gestation) – 33.8%. Considering the substantial size of Group 5, the further analysis of subgroups 5.1 and 5.2 was needed due to the different clinical management of these women. Among all women in the Group 5, only 100 women (31.1%) were in labor and the remaining 222 women (68.9%) from this group underwent caesarean section before the onset of labor. Subgroup 5.1 (women with one previous caesarean section) represents 83.2% of the total women of Group 5; among them, 89 women (33.2%) were in labor and 179 women (66.8%) underwent caesarean section before the onset of labor.
The second group according to the relative group contribution to the overall CS rate is represented by nulliparous women with a single cephalic pregnancy, ≥37 weeks of gestation, who had labor induced or were delivered by CS before labor (Group 2), with 14.7%. Of the total number of women from Group 2 who were delivered by caesarean section, 94 women (76.4%) were operated before labor onset (Group 2b), with a high relative group contribution to the overall CS rate – 11.3%.
Group 1 (nulliparous women with a single cephalic pregnancy, ≥37 weeks of gestation, in spontaneous labor) and Group 6 (all nulliparous women with a single breech pregnancy) contributed to the overall CS rate with 11.4% and 10.2%, respectively.
Group 4 (multiparous women without a previous caesarean section, with a single cephalic pregnancy, ≥37 weeks of gestation, who had labor induced or were delivered by caesarean section before labor) has a relative contribution of 6.7% to the total CS rate. Among all women from Group 4 who gave birth by caesarean section, 52 women (92.9%) were delivered by caesarean section before labor (Group 4b) which constitutes a relative contribution of 6.2% to the general CS rate.
Group 7 (all multiparous women with a single breech pregnancy, including women with previous caesarean section) and Group 8 (all women with multiple pregnancies, including women with previous caesarean section) had an approximately equal relative contribution of 5.6% and 5.7%, respectively, to the overall CS rate.
Group 10 (all women with a single cephalic pregnancy, <37 weeks of gestation, including women with previous caesarean sections) has a 4.8% contribution to the total CS rate. A detailed analysis of the group shows that 96 women (71.6%) had spontaneous onset of labor, 12 women had induced labor (9%), and 26 women (19.4%) had a pre-labor caesarean section.
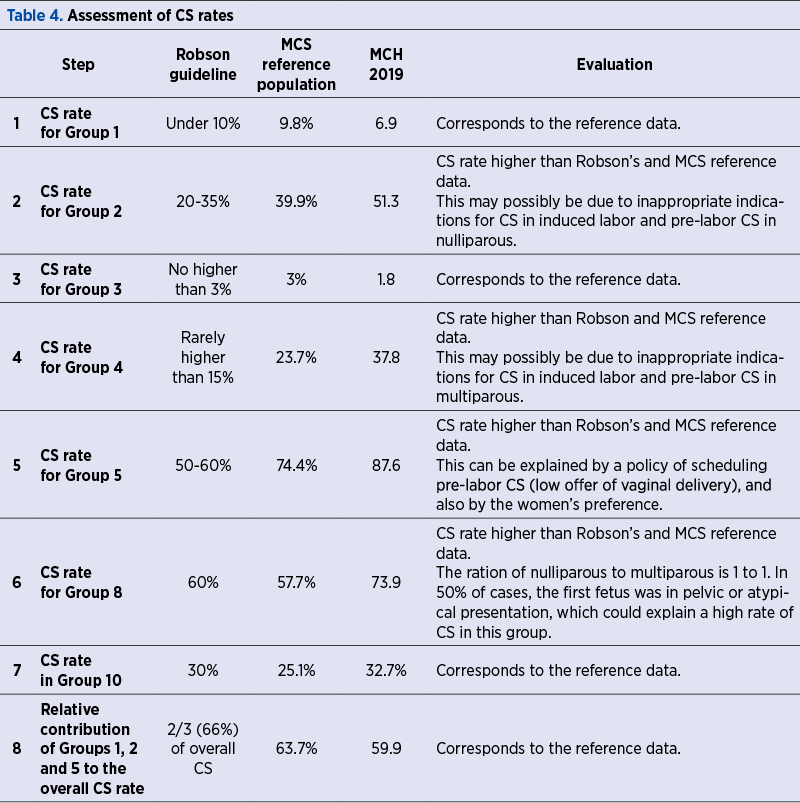
As a consequence of this analysis, we can state that 59.9% of the total number of caesarean sections performed in this period belong to the women from Groups 5, 2 and 1 (Table 3).
Discussion
Caesarean section is the main tool for improving maternal and fetal morbidity and mortality. It is also one of the main indicators of the quality of the maternal care service(9).
Despite all offered benefits, the caesarean section can be associated with serious maternal complications (sepsis, hemorrhage, anesthetic complications and even maternal death) as well as fetal complications(10), for this reason it is important to reduce unnecessary caesarean sections.
In order to ensure a clear and detailed evidence of caesarean sections, the Robson’s system of classification represents a helpful tool for every medical institution, due to its simplicity and exclusivity(9,11).
The results obtained in this study after analysis according to the 10 groups classification system were assessed and compared with the reference data proposed by Robson and the results of the WHO MCS on maternal and newborn health (Table 4).
In our study, Group 3 and Group 1 are the most prevalent groups in the obstetrical population. Similarly, studies from Brazil, Italy and Tanzania state that Groups 3 and 1 are the most representative obstetric groups(12-14).
The size of Groups 1 and 2 represents 37.7% and the ratio between these groups is 5.7 which is higher compared to the reference data (3.3%). Similarly, the ratio between the Group 3 size to the Group 4 size is 12.1 which is much higher than Robson’s and MCS reference data of 6.3(14-16). Both higher rates in our study likely indicate a need to increase the number of induced labors in these groups – singleton pregnancies, cranial presentation, ≥37 weeks, both for nulliparous and multiparous.
We infer the importance of the correct selection of women requiring induction of labor, so that, if it was selected an insufficient number of women who required induction of labor or delivered by CS before labor, the likelihood that these women will require a caesarean section at a later stage of the of labor is higher(15). In addition, the high rate of CS in Group 2 (51.3%) is not caused by the size of Group 2b (pre-labor CS) which is only 2.2% of the population, likely it is caused by a very small size of the Group 2a (3.4% of the population) and by poor success of induction with a high CS rate (20%) in this group. Similar arguments can be applied for Groups 3 and 4. The high rate of CS in Group 4 (37.8%) is not justified by the size of Group 4b, which represented only 1.2% of the population, but by the small size of Group 4a (2.2%) of the obstetrical population.
Group 5 is the third group in terms of group size and it is the first group with the highest relative contribution to the overall CS rate, which implies a high rate of caesarean section in previous years in the Republic of Moldova.
Only one third of Group’s 5 women were in labor, and among them 63% women were delivered by CS. A very high rate of caesarean sections in Group 5 (87.6%) markedly contrasts with the rates of 50-60% considered adequate by Robson and 74.4% according to WHO MCS(6-8).
Before making a recommendation for obstetricians to offer a vaginal delivery after caesarean section (VDAC) for more women, it is crucial to perform an assessment of the hospital’s ability to provide a safe labor process for women with a uterine scar after a previous caesarean section. Moreover, the lack of information about the previous caesarean delivery (how it was performed, the presence or not of intra- and postoperative complications) can be the cause of obstetrician’s hesitate to offer the possibility of an VDAC.
Conclusions
The strength of the Robson classification is its simplicity of use, clinical relevance and the possibility of using this classification by medical institutions from the Republic of Moldova, being an effective tool for analyzing the caesarean sections rate.
By implementing the Robson classification, we identified that groups contributing most of all to the total CS rate in our population are women with a history of caesarean section, followed by nulliparous women with a single pregnancy in cranial presentation, at term.
Group 1 and Group 2 require a more detailed analysis, to identify possible modifiable factors and to apply specific interventions in order to reduce the rate of first caesarean section in nulliparous women.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Gonzales GF, Tapia VL, Fort AL, Betran AP. Pregnancy outcomes associated with Cesarean deliveries in Peruvian public health facilities. Int J Women’s Health. 2013;5:637-45.
-
Betrán AP, Vindevoghel N, Souza JP, Gülmezoglu AM, Torloni MR. A systematic review of the Robson classification for caesarean section: what works, doesn’t work and how to improve it. PLoS One. 2014;9(6):e97769. doi: 10.1371/journal.pone.0097769.
-
Robson M, Murphy M, Byrne F. Quality assurance: The 10- Group Classification System (Robson classification), induction of labour, and cesarean delivery. Int J Gynaecol Obstet. 2015;131 Suppl 1:S23-7. doi: 10.1016/j.ijgo.2015.04.026.
-
Marian-Pavlenco A, Friptu V. Cesarean Section. Practical Guide. Chişinau, 2020. 114 p. ISBN 978-9975-56-758-9.
-
World Health Organization. Robson Classification: Implementation Manual. Geneva, 2017. p.56. ISBN 978-92-4-151319-7.
-
Souza JP, Betrán AP, Dumont A, de Muncio B, Gibbs Pickens C, Deneux-Tharaux C, et al. A global reference for caesarean section rates (C-Model): a multicountry cross-sectional study. BJOG. 2016;123:427–436.
-
Souza JP, Gülmezoglu AM, Vogel J, Carroli G, Lumbiganon P, Qureshi Z, et al. Moving beyond essential interventions for reduction of maternal mortality (the WHO Multicountry Surveyon Maternal and Newborn Health): a cross-sectional study. Lancet. 2013;18(38):1747-55.
-
Souza JP, Gulmezoglu AM, Carroli G, Lumbiganon P, Qureshi Z, WHOMCS Research Group. The World Health Organization multicountry survey on maternal and newborn health: study protocol. BMC Health ServRes. 2011;11:286.
-
World Health Organization. WHO statement on caesarean section rates, vol. WHO/RHR/15.02. Geneva: World Health Organization; 2015. (WHO/RHR/15.02).
-
Harrison MS, Pasha O, Saleem S, Ali S, Chomba E, Carlo WA, Garces AL, Krebs NF, Hambidge KM, Goudar SS. A prospective study of maternal, fetal and neonatal outcomes in the setting of cesarean section in low-and middle-income countries. Acta Obstet Gynecol Scand. 2017;96(4):410–20.
-
Robson MS. Classification of caesarean sections. Fetal Matern Med Rev. 2001;12(1):23–39.
-
Costa ML, Cecatti JG, Souza JP, Milanez HM, Gulmezoglu MA. Using a Caesarean Section Classification System based on characteristics of the population as a way of monitoring obstetric practice. Reprod Health. 2010;7:13.
-
Litorp H, Kidanto HL, Nystrom L, Darj E, Essen B. Increasing caesarean section rates among low-risk groups: a panel study classifying deliveries according to Robson at a university hospital in Tanzania. BMC Pregnancy Childbirth. 2013;13:107.
-
Triunfo S, Ferrazzani S, Lanzone A, Scambia G. Identification of obstetric targets for reducing cesarean section rate using the Robson Ten Group Classification in a tertiary level hospital. Eur J Obstet Gynecol Reprod Biol. 2015;189:91–5.
-
Sah S, Goel R, Goel JK. Analysis of caesarean section rate according to Robson’s criteria in tertiary care center. International Journal of Reproduction Contraception, Obstetrics and Gynecology. 2018;7(8):3060–4.
Articole din ediţiile anterioare
Infecţiile asociate plăgilor operatorii în pandemia de COVID-19: un studiu comparativ
Pandemia de COVID-19 a impus noi abordări, cu singurul scop de a prioritiza resursele în oferirea, în continuare, de servicii medicale calitative.
Sarcina cicatricială după operaţia cezariană – o continuă dilemă terapeutică. Serie de cazuri şi review al literaturii
Sarcina cicatricială după operaţie cezariană (CSP) este o tulburare iatrogenă care pune viaţa în pericol, cu o incidenţă tot mai mare, din cauza cr...
Placenta accreta – o preocupare tot mai mare în epidemia de operaţii cezariene
În ultimii ani, este de remarcat creşterea îngrijorătoare a numărului de operaţii cezariene efectuate la nivel global. Această intervenţie urmează ...
Cine stabileşte indicaţia operaţiei cezariene? Studiu transversal într-o maternitate de nivel III, despre profilul doctorilor şi al pacientelor la naştere
Având în vedere cât de frecventă este acum operaţia cezariană, obiectivele noastre sunt: 1) să analizăm felul în care româncele doresc să nască şi ...