Background and objectives. Gastroschisis is a low-prevalence fetal anomaly with an excellent long-term prognosis and survival rates if early and adequate management is performed. It can be easily identified both prenatally and postnatally. It is described depending on the location of the defect, most often to the right side of a normally inserted umbilical cord. Prenatal ultrasound scans proved to be fundamental for the early diagnosis and for the prediction of likelihood complications, such as bowel atresia. Case report. We hereby present a fetus with gastroschisis who was diagnosed in the second trimester of pregnancy. After delivery, the newborn received proper surgical care and had a favorable outcome. At 4 years old, the baby had regular follow-ups as an outpatient, receiving full enteral nutrition. No hepatic damage was detected. We underline that there have been significant improvements in the outcome of newborns diagnosed with gastroschisis in the last 30 years, due to the in utero detection of this anomaly and to standardized neonatal care. Materials and method. We performed a systematic review of the available literature from 2013 to 2023 using PubMed and Google Scholar databases to search for published studies regarding ultrasound diagnosis and surgical management of gastroschisis according to PRISMA guidelines. The following search terms were used: “gastroschisis”, “ultrasound”, “neonatal surgery”. Results. After the appropriate screening, we selected 15 papers. The diagnosis was first reached in one case in the first trimester, in seven cases during the second trimester and, respectively, two cases in the third trimester. In one case, the ultrasound showed normal previous scans, and for four cases, there were no available data for the gestational age at diagnosis. Surgery was performed on the first day of life for 11 neonates, and on the third, fourth, eighth and thirty-eighth days for the others. Conclusions. Multidisciplinary teams, including maternal-fetal medicine specialists, neonatologists and pediatric surgeons, are highly advised. This assures the best prenatal counseling and postnatal care.
Successful management of gastroschisis – case report and literature review
Managementul eficient al gastroschizisului – prezentare de caz şi review al literaturii
First published: 22 decembrie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ObsGin.71.4.2023.9128
Abstract
Rezumat
Context şi obiective. Gastroschizisul este o anomalie fetală cu o prevalenţă redusă. Ratele de supravieţuire şi prognosticul pe termen lung sunt excelente dacă intervenţia este precoce şi dacă se adoptă o conduită adecvată. Malformaţia se recunoaşte uşor, atât în perioada prenatală, cât şi postnatal. Se clasifică în funcţie de partea afectată, cel mai frecvent defectul fiind situat de partea dreaptă a inserţiei cordonului ombilical. Identificarea ecografică prenatală are o importanţă critică atât în diagnosticul precoce, cât şi în predicţia riscului anumitor complicaţii (precum atrezia intestinală). Prezentare de caz. Prezentăm un caz de gastroschizis diagnosticat în al doilea trimestru de sarcină. După naştere, fătul a primit îngrijire chirurgicală adecvată şi a evoluat favorabil. În prezent, copilul are 4 ani, fiind supravegheat în serviciul ambulatoriu la intervale regulate şi având o alimentaţie exclusiv enterală. Nu a dezvoltat complicaţii hepatice. În ultimii 30 de ani s-au înregistrat progrese semnificative, iar prognosticul nou-născuţilor cu gastroschizis s-a îmbunătăţit mult. Cel mai important rol le au diagnosticul prenatal şi standardizarea îngrijirii postnatale. Materiale şi metodă. Autorii au realizat o revizie sistematică a literaturii publicate între 2013 şi 2023 în bazele de date PubMed şi Google Scholar, respectând criteriile PRISMA. Au fost selectate studii ce includ atât descrierea datelor ecografice în perioada prenatală, cât şi conduita chirurgicală. În motoarele de căutare au fost folosiţi termenii „gastroschizis”, „examinare ecografică” şi „intervenţie chirurgicală”. Rezultate. După studierea amănunţită a literaturii disponibile, au fost selectate 15 publicaţii. Diagnosticul a fost precizat în primul trimestru într-un caz, în şapte cazuri acesta a fost precizat în al doilea trimestru, iar în două cazuri, în cel de-al treilea trimestru de sarcină. Într-un caz, examinarea ecografică prenatală a fost negativă, iar în patru cazuri nu au fost disponibile informaţii cu privire la vârsta gestaţională la care s-a precizat diagnosticul. Intervenţia chirurgicală a fost practicată în prima zi de viaţă în 11 din cazurile publicate, respectiv în zilele 3, 4, 8 şi 33 în celelalte. Concluzii. Se recomandă managementul în echipe multidisciplinare ce includ specialişti în medicină materno-fetală şi în chirurgia pediatrică, dar şi neonatologi. Aceasta permite optimizarea consilierii prenatale şi a conduitei în perioada postnatală.
Introduction
Gastroschisis is a paraumbilical full-thickness abdominal wall defect, associated with protrusion of the bowel through the defect. This defect is usually observed to the right of the navel(1), involving in all cases the small intestine(2) and sometimes the stomach, colon or gonads(1). The eviscerated structures are not covered by membranes, and they are exposed to the amniotic fluid (and external environment – after delivery), increasing the risk of infections and injuries(2). The cited risk factors for gastroschisis are young maternal age, smoking, drug use, and maternal infections(3). A genetic condition is rarely associated, and fetal karyotyping is not routinely offered. However, pregnancies complicated with gastroschisis have an increased risk of developing intrauterine growth restriction, preterm labor, intrapartum fetal heart rate abnormalities, and increased hospitalization length(4). There is also an increased risk of intrauterine fetal demise(4).
The spread of routine first-trimester nuchal scans with the purpose of screening for chromosomal abnormalities greatly improved the detection of fetal structural defects. Nowadays, the detection rate for gastroschisis during routine first-trimester scans is high(5).
We report a case of a preterm newborn with right-sided gastroschisis. The defect was diagnosed antenatally. The baby had the benefits of immediate (first day of life) active surgical management, with a successful outcome.
Case report
A 19-year-old pregnant woman was referred to the Prenatal Diagnosis Unit in the Emergency County Hospital of Craiova for the suspicion of fetal abdominal wall defect.
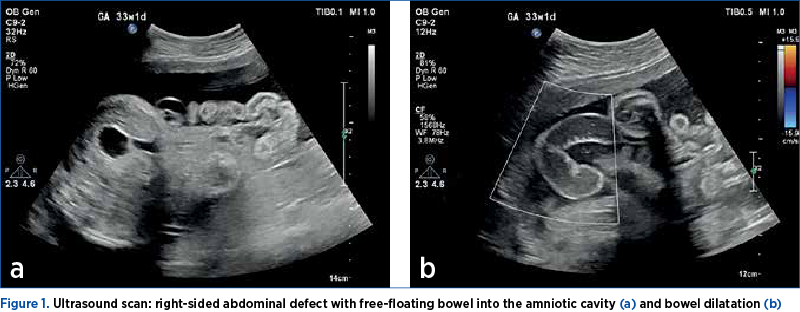
The patient was a smoker (one pack per day) and presented with no previous obstetric history. She had a late booking and registration (no previous prenatal care). At 29 weeks and 3 days of gestation, the ultrasound report described a live fetus with an estimated fetal weight of 1480 g. The fetus presented a paraumbilical abdominal wall defect to the right side of the midline, with herniation of the free-floating bowel into the amniotic cavity: fetal gastroschisis (Figure 1). The amniotic fluid volume was normal.
The patient was assessed by a multidisciplinary team (pediatric surgeon, neonatologist and maternal-fetal specialist), and specialized tailored postnatal care was offered. The patient expressed interest in a full spectrum of neonatal interventions.
The steroid prophylactic treatment was administered. The patient presented with preterm labor at 35 WA, and the team performed an emergency caesarean section delivery. The preterm newborn was a baby girl weighing 2080 g, with an Apgar score of 8 at 5 minutes.
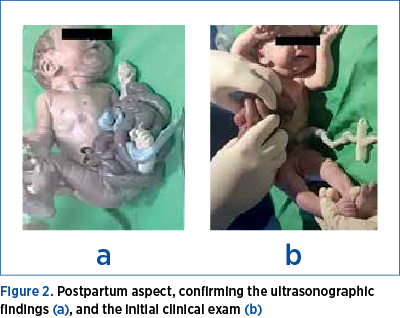
The neonatologist described the eviscerated bowel to be mild edematous, and no other associated anomaly was diagnosed postpartum (Figure 2).
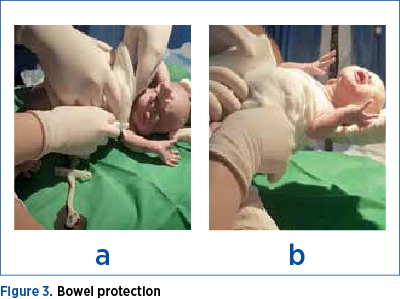
Intensive neonatal care was initiated immediately after delivery to maintain physiological homeostasis: intravenous fluids, thermoregulation, and bowel protection (Figure 3). Also, a nasogastric tube was ensured to facilitate intestinal decompression.
The newborn was managed in the operating room by a multidisciplinary team: pediatric surgery and neonatology.
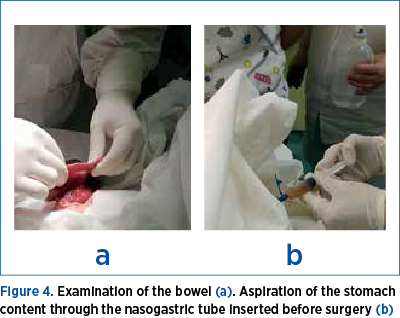
During the following hour, the baby was transferred to the pediatric surgery department. The intervention was soon performed. The bowel was inspected at the time of reduction for obstructing bands, perforation or atresia (Figure 4a). A nasogastric tube was inserted into the stomach to keep it empty in order to prevent choking on or breathing in stomach contents into the lungs (Figure 4b). The team opted to return the exposed bowel to the abdominal cavity, with a minimal intestinal injury and without increasing the intraabdominal pressure. In the end, the wall defect was completely repaired.
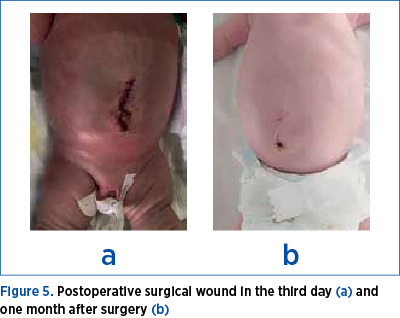
The patient required intubation with mechanical ventilation the following four postoperative days. She had a slow favorable evolution. The intestinal movement was resumed spontaneously on the third day after surgery. General nutrition was resumed on the nineth day. After one month, the patient was discharged in very good condition, weighing 2500 g (Figure 5).
Two weeks after the discharge, the newborn presented important abdominal distension, vomiting, and lack of bowel movements for 24 hours. She was readmitted with the suspicion of ileus and treated with antibiotics and parenteral nutrition for seven days. All symptoms and clinical signs improved with conservative management. Currently, the baby girl has excellent development, with no further complications.
Materials and method
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for reporting systematic reviews, we performed a search on PubMed and Google Scholar databases, using the keywords “gastroschisis”, “ultrasound” and “neonatal surgery”.
We included in our study manuscripts reporting cases diagnosed with gastroschisis that received prenatal care and surgical treatment. We establish the exclusion criteria: uncertain diagnosis, vanishing or spontaneous repair of the defect, chromosomal diseases, pregnancy termination, ongoing pregnancies, and treatments other than surgery (e.g., silo placement). After a first screening based on titles and abstracts, all selected papers were assessed based on the full text to choose the relevant publications. Two authors carried out this review independently.
The informed consent was obtained from the patient for the publication of the case report.
Results
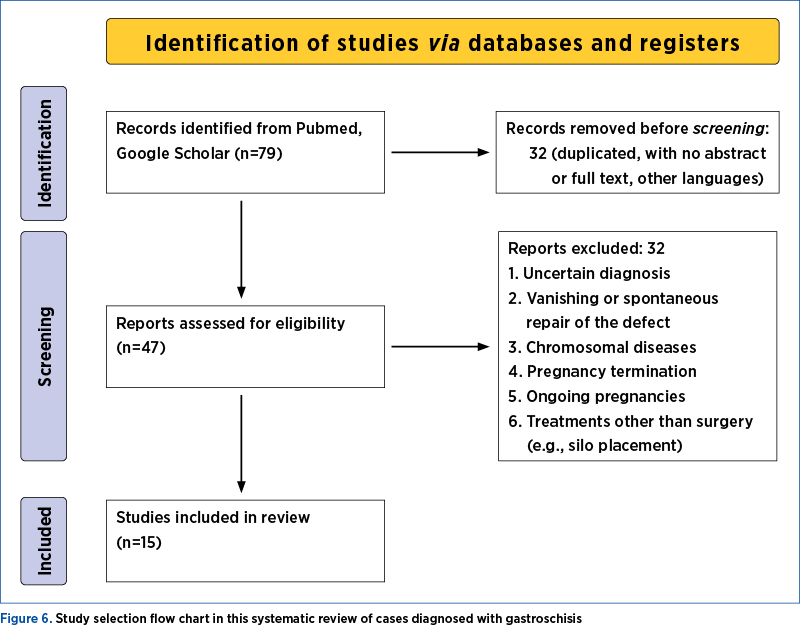
We identified 79 articles that were manually examined in accordance with the inclusion and exclusion criteria. After the exclusion of articles that contained no postnatal information on patients with gastroschisis and the exclusion of articles with no abstract or full text, duplicates, or other languages, 32 articles remained. A further assessment based on the full text led to the exclusion of 17 papers.
Data related to maternal age, parity, gestational age at diagnosis, ultrasound and MR-associated findings, delivery, the characteristics of the fetus, surgery, and neonatal outcomes were extracted. As seen in Tables 1 and 2, we were not able to collect all the data according to our objective because in some cases there were no mentions in the description(6-20).
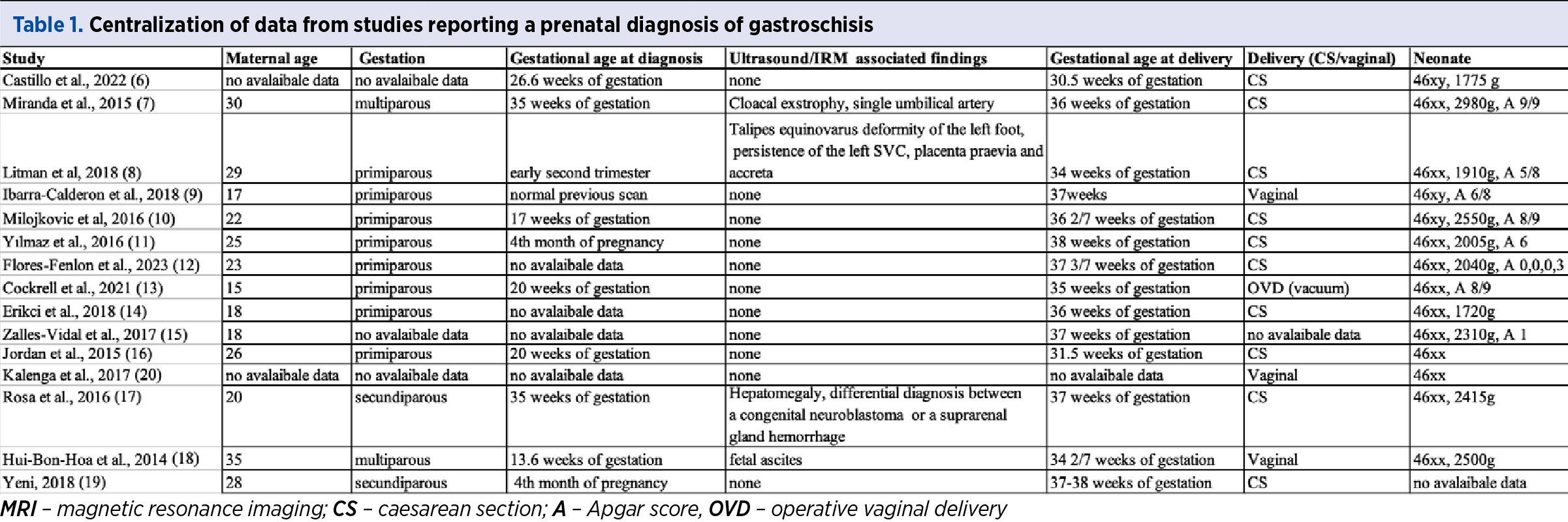
The mean maternal age at diagnosis was 23.5 years old, with a 5.7 standard deviation. Two studies did not report the maternal age(6,20).
Three studies did not provide data about parity(6,15,20). Eight out of 12 patients (66.66%) were primiparous, two out of 12 patients (16.66%) were secundiparous, and two out of 12 patients (16.66%) were multiparous.
Four out of 15 studies did not mention information about the gestational age at diagnosis(12,14,15,20). One study reported a normal previous scan(9). In 70% of cases, the diagnosis was proposed in the second trimester, in 20% of the cases, in the third trimester, and 10% in the first trimester.
Eleven out of 15 studies (73.33%) did not report any other ultrasound or MRI-associated findings.
One study did not report the gestational age at delivery(20). Also, 57.14% of the newborns were premature, and 42.86% were born at term.
One study did not report the delivery mode(15). In 71.43% of cases, a caesarean section was performed, while 28.57% were vaginal deliveries.
In terms of gender distribution, there was a predominance of female newborns diagnosed with gastroschisis, representing 78.57%, while 21.43% were male newborns. One study did not report gender(19). For the studies that reported birth weight, the mean weight was 2220 g, with a standard deviation of 378.65.
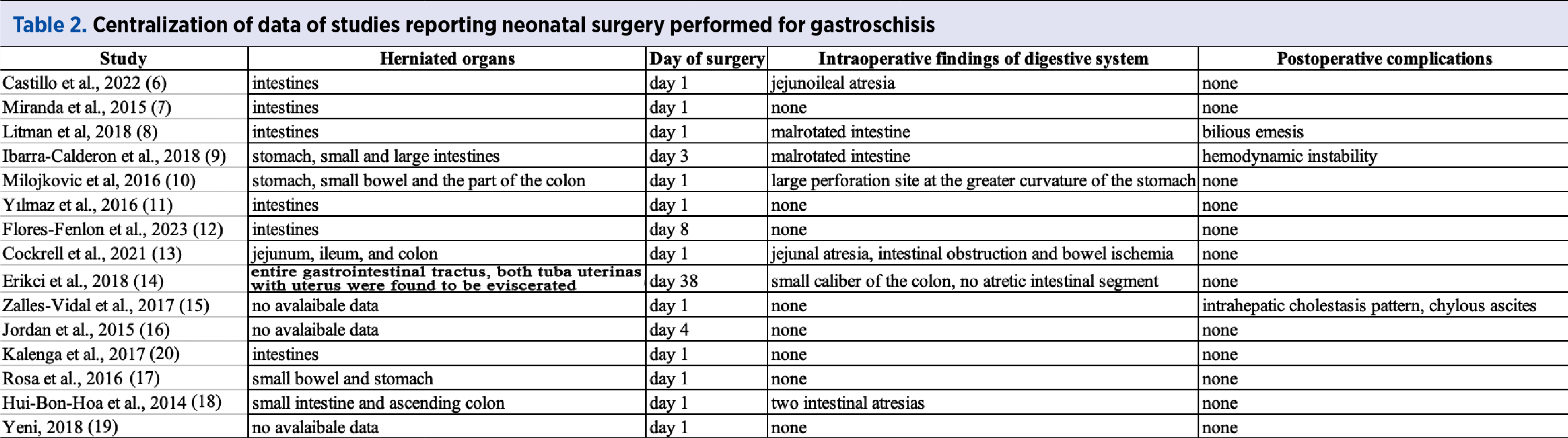
Three out of 15 studies did not report the herniated organs. Eleven cases out of 12 (91.67%) reported as herniated organs parts of the digestive tube, while one case (8.33%) reported herniation of both parts of the digestive tube and the internal genital organs.
Eleven out of 15 newborns (73.33%) were operated on the first day of life.
Seven out of 15 studies (46.67%) reported intraoperative complications associated with gastroschisis: two cases associated with bowel malrotation, three cases reported intestinal atresia, one case with a large stomach perforation, and one case reported a smaller caliber of the colon.
Twelve out of 15 surgeries (80%) did not encounter any postoperative event.
Discussion
The International Clearinghouse for Birth Defects Surveillance and Research defines gastroschisis as “a congenital malformation characterized by visceral herniation usually right-side abdominal wall defect to an intact umbilical cord and not covered by a membrane”(21).
The cause of gastroschisis is incompletely understood. Gastroschisis is caused by a failure of the formation and development of the ventral body wall during embryogenesis, resulting in herniation of the bowel.
The rate of gastroschisis has increased significantly, and it seems to be associated with young maternal age, with the highest prevalence among mothers aged below 20 years old(3). Our case also falls in this age group. Approximately 10% of cases are associated with other non-gastrointestinal pathologies, and in up to 25% of cases, additional gastrointestinal problems are present. In our case, the gastroschisis was isolated – no gastrointestinal associations were detected, or other systems’ defects. The karyotype is reported to be abnormal in 1% of cases, usually in the setting of associated abnormalities(22). In our case, karyotyping was not performed, due to the absence of associated structural anomalies and the normal phenotype.
Gastroschisis can be accurately diagnosed by a prenatal ultrasound performed in the second trimester(23). Usually, the ultrasound scan detects a defect to the right of the umbilical cord, and free-floating bowel loops are visualized. After the diagnosis, we checked the fetal growth and the amniotic fluid volume every three to four weeks, according to current commendations(24). The bowel exposed to amniotic fluid for a long period of time can become thickened and dilated. In our case, the good quality of the exposed bowels was preserved. Oligohydramnios may be related to fetal growth restriction and can be a risk factor for cord compression, while polyhydramnios may predict bowel atresia(25). Fortunately, in our case, there were no such complications. Growth restriction in fetuses with abdominal wall defects usually indicates increased adverse neonatal outcomes(26). Our fetus maintained a normal growth curve in utero, paving the way to a good outcome postpartum.
It is advisable to offer prenatal care by a group of specialists, including a maternal-fetal medicine specialist, neonatologist and pediatric surgeon. This assures patient-specific counseling before delivery. The mean gestational age for spontaneous delivery in women carrying infants with gastroschisis is 36 weeks of gestation(27). We performed an emergency caesarean section at 35 weeks, due to the spontaneous onset of preterm labor.
The management of the newborn must begin in the delivery room. The fluid loss through the exposed bowel is 2.5 times higher than the amount of a healthy newborn(28). Initial management includes protecting the exposed bowel by placing the lower half of the infant into a bowel bag. This maneuver allows the protection of the bowel, as well as the visualization of the blood flow and perfusion of the bowel. An orogastric tube should be inserted to decompress the stomach(22). The extended team performed all these recommended interventions.
Compared with infants born with other abdominal wall defects, infants born with gastroschisis have the most favorable prognosis, with excellent long-term outcomes(29). The overall survival rate is 98% in live newborns(30). The need for surgery beyond the neonatal period is reported to be significant, with approximately 25% of patients requiring surgical treatment for a gastroschisis-related complication, most commonly bowel obstruction, within the first year of life(31). In our case, these short-term and long-term complications were absent.
Conclusions
Gastroschisis is a rare congenital defect. It implies prenatal diagnosis by specialized practitioners and timely referral of the mother (before birth) to a tertiary unit with pediatric surgery facilities. Routine preterm delivery or elective caesarean section in the absence of obstetric indications remains controversial, as their efficiency to prevent adversities lacks scientific proof. After delivery, the initial therapeutic goals in the neonatal intensive care unit are represented by the maintenance of physiologic homeostasis with intravenous fluids, respiratory support if required, thermoregulation, and bowel protection. The goal of surgical treatment of gastroschisis is the reduction of the intestines and abdominal closure, with the avoidance of physiologically intolerable increases in intraabdominal pressure. This management avoids the complications and ensures a favorable outcome. Nowadays, the short- and long-term prognosis of isolated gastroschisis is excellent.
Corresponding author: Ştefania Tudorache, e-mail: stefania.tudorache@gmail.com
Conflict of interest: none declared
Financial support: none declared
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
-
Frolov P, Alali J, Klein MD. Clinical risk factors for gastroschisis and omphalocele in humans: a review of the literature. Pediatr Surg Int. 2010;26(12):1135-48.
-
Van Dorp DR, Malleis JM, Sullivan BP, Klein MD. Teratogens inducing congenital abdominal wall defects in animal models. Pediatr Surg Int. 2010;26(2):127-39.
-
Jones AM, Isenburg J, Salemi JL, Arnold KE, Mai CT, Aggarwal D, et al. Increasing Prevalence of Gastroschisis - 14 States, 1995-2012. MMWR Morb Mortal Wkly Rep. 2016;65(2):23-6.
-
Lausman AY, Langer JC, Tai M, et al. Gastroschisis: what is the average gestational age of spontaneous delivery? J Pediatr Surg. 2007;42(11):1816-21.
-
Drăguşin RC, Şorop-Florea M, Pătru CL, Zorilă L, Marinaş C, Cernea N, Iliescu DG. Chapter 10. Fetal Abdominal Wall Defects. In: Tudorache Ş (Editor). Congenital Anomalies. Rijeka: IntechOpen; 2017.
-
Castillo-Clavijo JL, Gálvez-Salazar PF, Ángel-Correa M, Montañez-Azcárate V, Palta-Uribe DA, Figueroa-Gutiérrez LM. Complex gastroschisis with apple peel jejunoileal atresia, primary closure, and Santulli procedure as a surgical alternative. Case report. Int J Surg Case Rep. 2022;94:107095.
-
Miranda ME, Piçarro C, Campos BA, Camelo AA, Belêsa FdA, Tatsuo ES, et al. Cloacal exstrophy associated with gastroschisis: Case report of a rare association with favorable outcome. Journal of Pediatric Surgery Case Reports. 2015;3(3):107-10.
-
Litman EA, Robinson TD, Munshi UK, Whyte C. Left-sided gastroschisis: A case report and review of the literature. Journal of Pediatric Surgery Case Reports. 2018;36(C):50-3.
-
Ibarra-Calderón R, Gutiérrez-Montufar OO, Saavedra-Torres JS, Zúñiga Cerón LF. Gastroschisis. Case report and management in primary care services. Case Reports. 2018;4(1):10-18.
-
Marinovic VM, Lukac ML, Mikovic Z, Grujic B, Stojanovic A, Sabbagh D, et al. Gastroschisis with gastric perforation and jejunal stenosis A rare association of anomalies. Ann Ital Chir. 2016;87:263-7.
-
Yılmaz J İİ, İnan M. A case report: Gastroschisis. Turk Med Stud. 2016;3:22-5.
-
Flores-Fenlon N, Shafer G, Awan S, Ahmad I. Therapeutic Hypothermia Treatment for an Infant with Hypoxic-Ischemic Encephalopathy and Gastroschisis: A Case Report. AJP Rep. 2023;13(1):e17-e20.
-
Cockrell H, Shaw T, Morris MW. Closed Gastroschisis: A Rare Abdominal Wall Defect. Am Surg. 2022;88(3):544-6.
-
Erikci V, Mert M, Özdemir T, Köylüoğlu G. Gastroschisis in a Premature Infant: A Case Report and Review of Literature. EC Paediatrics. 2018;7:5.
-
Zalles-Vidal CR, Penarrieta-Daher A, Ibarra-Rios D, Fernandez-Portilla E, Bracho-Blachet E. Chylous Ascites in a Newborn with Gastroschisis. Case Report. J Neonatal Surg. 2017;6(1):16.
-
Jordan MA, Montezuma SR. Septo-optic dysplasia associated with congenital persistent fetal vasculature, retinal detachment, and gastroschisis. Retin Cases Brief Rep. 2015;9(2):123-6.
-
Rosa RF, Michelon L, Masiero A, Faria AE, De Souza VF, Dietrich C, et al. Gastroschisis in a fetus with a congenital neuroblastoma: Association or coincidence? Birth Defects Res A Clin Mol Teratol. 2016;106(3):208-12.
-
Hui-Bon-Hoa I, Timmons J, Rypens F, Piché N, Audibert F. P11.19: Closing gastroschisis: a case report with unusual antenatal ascites and literature review. Ultrasound in Obstetrics & Gynecology. 2014;44(S1):247-8.
-
Yeni C. EP06.30: Case report: gastroschisis. Ultrasound in Obstetrics & Gynecology. 2018;52(S1):218-218.
-
Kalenga NC. Left-Sided Gastroschisis: Case Report and Some Anatomic and Technical Considerations. Open Access Journal of Surgery. 2017;2.
-
International Clearinghouse for Birth Defects Monitoring Systems. Annual report. San Francisco, CA: The Clearinghouse; 1982.
-
Rentea RM, Gupta V. Gastroschisis. In: StatPearls. Treasure Island (FL): StatPearls Publishing; April 10, 2023.
-
Islam S. Clinical care outcomes in abdominal wall defects. Curr Opin Pediatr. 2008;20(3):305-10.
-
Amin R, Domack A, Bartoletti J, Peterson E, Rink B, Bruggink J, et al. National Practice Patterns for Prenatal Monitoring in Gastroschisis: Gastroschisis Outcomes of Delivery (GOOD) Provider Survey. Fetal Diagn Ther. 2019;45(2):125-30.
-
Japaraj RP, Hockey R, Chan FY. Gastroschisis: can prenatal sonography predict neonatal outcome? Ultrasound Obstet Gynecol. 2003;21(4):329-33.
-
Nicholas SS, Stamilio DM, Dicke JM, Gray DL, Macones GA, Odibo AO. Predicting adverse neonatal outcomes in fetuses with abdominal wall defects using prenatal risk factors. Am J Obstet Gynecol. 2009;201(4):383 e1-6.
-
Overcash RT, DeUgarte DA, Stephenson ML, Gutkin RM, Norton ME, Parmar S, et al. Factors associated with gastroschisis outcomes. Obstet Gynecol. 2014;124(3):551-7.
-
Zalles-Vidal C, Penarrieta-Daher A, Bracho-Blanchet E, et al. A Gastroschisis bundle: effects of a quality improvement protocol on morbidity and mortality. J Pediatr Surg. 2018;53(11):2117-22.
-
Lepigeon K, Van Mieghem T, Vasseur Maurer S, Giannoni E, Baud D. Gastroschisis - what should be told to parents? Prenat Diagn. 2014;34(4):316-26.
-
Fullerton BS, Velazco CS, Sparks EA, Morrow KA, Edwards EM, Soll RF, et al. Contemporary Outcomes of Infants with Gastroschisis in North America: A Multicenter Cohort Study. J Pediatr. 2017;188:192-7.e6.
-
Friedmacher F, Hock A, Castellani C, Avian A, Höllwarth ME. Gastroschisis-related complications requiring further surgical interventions. Pediatr Surg Int. 2014;30(6):615-20.
Articole din ediţiile anterioare
Cystic hygroma presenting as an isolated malformation – case report and literature review
Nuchal translucency (NT) is the ultrasound observation of subcutaneous fluid accumulation at the back of the fetal neck. When this accumulation be...
Screeningul ecografic în al treilea trimestru al sarcinii
Ultrasound screening for pregnancy abnormalities in the third trimester is a specialized investigation which should be considered a routine/standar...
Endometrioma – the tip of the iceberg?
About 10% of women of reproductive age have endometriosis, a chronic illness that may cause serious morbidity, being ultimately a major public heal...
Anatomic landmarks in radical hysterectomy
Cervical cancer provides one of the few examples of controversial treatment management throughout medical history. Radical hysterectomy was first d...