Among urinary tract tumors, renal cancer is the most common, and regarding histopathological subtype, the clear cell type ranks first. We present the case of a patient who developed two types of solid tumors over an 11-year period. This case also highlights the role of preexisting renal lesions in the development of this cancer, the impact of early intervention on the subsequent course of the disease, as well as the importance of a multidisciplinary team in the treatment of patients with metastatic kidney cancer. Furthermore, despite the complications arising from metastatic renal cancer, the patient maintained a preserved quality of life almost two years after diagnosis.
CASE PRESENTATION
Diffuse large B-cell lymphoma and metachronous metastatic renal cancer – a case report
Limfom non-Hodgkin difuz cu celule B şi cancer renal metastatic metacron – prezentare de caz
Goga Iolanda ,
Cioc Enache ,
Boghici Elena-Monica ,
Moraru Mihaela ,
Nichita Monica-Adriana,
Dumitrescu Elena ,
Pirlea Andrei-Daniel ,
Zob Daniela-Luminiţa
First published: 27 martie 2024
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/OnHe.66.1.2024.9378
Abstract
Rezumat
Dintre tumorile tractului urinar, cancerul renal este cel mai frecvent, iar în ceea ce priveşte subtipul histopatologic, cel cu celule clare ocupă primul loc. Prezentăm cazul unui pacient care, pe parcursul a 11 ani, a dezvoltat două tipuri de tumori. Acest caz evidenţiază, de asemenea, rolul leziunilor preexistente de la nivel renal în dezvoltarea acestui cancer, impactul intervenţiei precoce asupra evoluţiei ulterioare a bolii, precum şi importanţa echipei multidisciplinare în tratamentul pacienţilor cu cancer renal metastatic. De asemenea, în ciuda complicaţiilor apărute ca urmare a unui neoplasm renal metastatic, pacientul a rămas după aproape doi ani de la diagnostic cu o calitate a vieţii păstrată.
Introduction
The kidney represents a site for both primary tumors and secondary metastases from neoplasms with other primary location. Clear cell cancers account for approximately 85% of renal tumors. These patients may have various clinical presentations, such as hematuria and lower back pain, but many of them can be asymptomatic until advanced stages of the disease(1). It has been demonstrated that clear cell renal neoplasm is associated with a multitude of risk factors, among which male sex appears to be more commonly affected, but in most cases, localized disease has been the most common form of disease extension presentation(2).
Case report
A 66-year-old patient presented for the first time to the emergency room in 2011 with digestive symptoms, such as nausea, vomiting, and abdominal pain. Consequently, an upper digestive endoscopy was performed, and the tumor formation located in the gastric area was biopsied. Following histopathological and immunohistochemical examination, the patient was diagnosed with diffuse large B-cell non-Hodgkin malignant lymphoma. The computed tomography scan at that time highlighted a lesion in the right kidney, raising suspicion of angiomyolipoma or metastasis. The patient underwent polychemotherapy and biological therapy, and a surgical intervention was performed – respectively, total gastrectomy with gastro-jejunal anastomosis.
The patient remained under surveillance with periodic imaging assessments, during which, from 2012 to 2016, the renal tumor formation remained stable in terms of size. Surgical excision of the renal lesion was proposed, but the patient refused it.
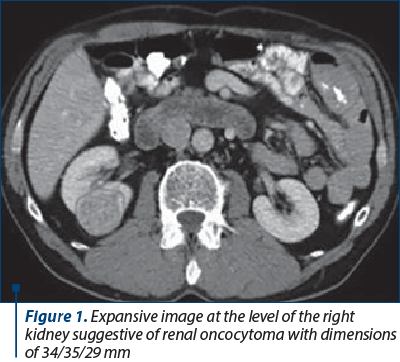
The CT scan from 2016 revealed an increase in the size of the renal formation, suggestive of renal oncocytoma (Figure 1).
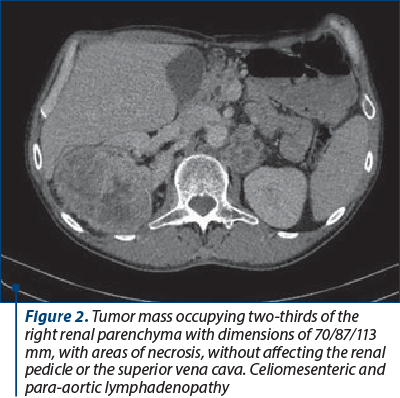
Upon repeated imaging in 2022, the cerebral-thoracic-abdominal-pelvic CT scan highlighted a large tumor formation in the right kidney, measuring 70/87/113 mm, along with celiomesenteric and para-aortic lymphadenopathy (Figure 2),
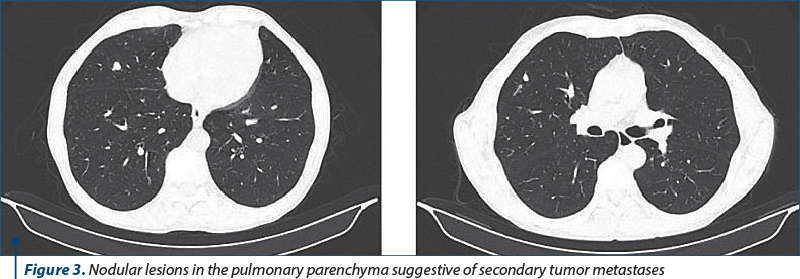
pulmonary nodular lesions, and right mediastinal lymphadenopathy, all suggestive of secondary metastases (Figure 3).
Right nephrectomy was performed, along with biopsy of a lung nodule. Both the resected specimen and the biopsy were examined histopathologically and immunohistochemically, confirming the diagnosis of stage IV clear cell renal carcinoma. Despite multiple secondary determinations, the patient was asymptomatic and had a very good performance status.
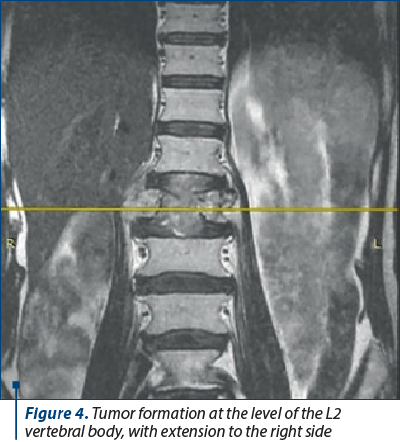
Thus, the patient was classified as intermediate risk and started the combined treatment, immunotherapy with a tyrosine kinase inhibitor, avelumab + axitinib. Over the following months, the oncological disease remained stable, but in March 2023 the patient presented with significant lower back pain, motor deficit in the lower limbs, and paresthesia. MRI examination revealed a new bony lesion located at the L2 level (Figure 4),
therefore surgical intervention was performed, involving L2 corpectomy and L1/L2 and L2/L3 discectomy, with complete removal of the tumor formation and reconstruction using acrylic cement for the L2 vertebral body (Figure 5).

The histopathological examination confirmed the vertebral metastasis with discal extension of clear cell carcinoma, measuring 11/10/2 cm. The postoperative evolution was remarkable, with complete remission of the motor deficit, and the patient also underwent palliative radiotherapy at this level. Follow-up imaging revealed disease progression through recurrence in the right nephrectomy bed and the appearance of a retroperitoneal tumor formation encompassing the L2 vertebra and involving the vertebroplasty material at this level. Considering the progression of the oncological disease, the decision was to change the treatment line with cabozantinib and a monoclonal antibody targeting RANKL, a treatment that the patient continues. Currently, the cranial-thoracic-abdominal-pelvic CT scan with contrast shows stable oncological disease, and the patient has an overall survival of 22 months from diagnosis to present, with an ECOG performance status of 0, despite metastatic disease.
Discussion
There are several risk factors associated with renal cancer, such as smoking, diabetes mellitus, obesity, preexisting renal cystic lesions, hypertension, previous chemotherapy, and exposure to occupational toxins(3). The patient had a history of smoking for approximately 20 years, quitted smoking at a young age, and had grade I hypertension. However, the most important factor is that the patient presented with a renal lesion since 2011, probably benign at that time, which evolved slowly and transformed into a tumor.
The definitive diagnosis of a tumor formation is based on histopathological examination. Studies have shown that renal oncocytomas behave benignly, especially in cases where they are below 4 cm, and active surveillance is safe in these cases. However, there have been cases where patients developed metastatic disease when renal tumors were larger or symptomatic(4). Additionally, there were cases reported where the histopathological results showed that a renal tumor can be both clear cell renal carcinoma and oncocytoma at the same time(5). In this case, surgical intervention performed at the appropriate time would have provided a definitive diagnosis and most likely would have changed the course of the disease.
From the patient’s history, we also note the diagnosis of diffuse large B-cell non-Hodgkin gastric lymphoma, which may also represent a risk factor for the development of clear cell renal cancer. A multivariate analysis with age, race and sex identified that white males had a higher incidence of developing this type of cancer after non-Hodgkin lymphoma(6). Additionally, it has been demonstrated that not only non-Hodgkin lymphoma can lead to the development of subsequent clear cell renal neoplasm, but also other solid tumors, such as colorectal cancer, bladder cancer, lung cancer, prostate cancer, and breast cancer. After the diagnosis of these tumors, the highest risk of developing renal cancer is within the first five years(7). The possible causes may include careful patient surveillance, treatment effects, genetic associations, and possibly other factors involved, especially when there is a risk of developing a second cancer after five years. In the case of the presented patient, it cannot be precisely determined at what interval the second neoplasm appeared, because it was diagnosed after approximately 11 years, already in a metastatic stage.
After pulmonary metastases, bone metastases are the second most frequent site of metastasis, followed by metastases to lymph nodes, liver, adrenal glands, and brain metastases(8). In the case of bone metastases, palliative surgical intervention plays a very important role if the patient presents with spinal cord compression syndrome or unstable spinal column, achieving consolidation and even remission of neurological and painful symptoms. Generally, the best results are obtained in cases where combined therapy is practiced – i.e., surgical intervention followed by postoperative palliative radiotherapy, compared to radiotherapy as a single treatment modality(9). Regarding the presented patient, he had maximal benefit in terms of performance status following multimodal therapy, with the remission of pain syndrome, motor deficit, and the resumption of daily activities.
Conclusions
We reported the case of a patient with stage IV clear cell renal carcinoma, with several common risk factors for this type of cancer, but the particularity is that, over a certain period of time, he developed two different types of tumors.
This case highlights the complexity of the pathology and the challenges regarding diagnosis and treatment, as well as the importance of patient’s monitoring both from an imaging and clinical perspective, as any change in performance status or the appearance of new symptoms may indicate the presence of new secondary determinations. In our case, prompt intervention for vertebral bone metastasis had a positive impact on the patient’s quality of life.
Corresponding author: Daniela-Luminiţa Zob E-mail: danielazob@yahoo.com
Conflict of interest: none declared.
Financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY licence.

Bibliografie
-
Atkins MB. UpToDate. Clinical manifestation, evaluation and staging of renal cell carcinoma. Published: Dec 15, 2023, Accesed: Feb 24, 2024. https://www.uptodate.com/contents/clinical-manifestations-evaluation-and-staging-of-renal-cell-carcinoma
-
Atkins MB, Bakouny Z, Choueiri TK. UpToDate. Epidemiology, pathology, and pathogenesis of renal cell carcinoma, Published: Mar 03, 2023, Accesed: Feb 24, 2024. https://www.uptodate.com/contents/epidemiology-pathology-and-pathogenesis-of-renal-cell-carcinoma
-
Kabaria R, Klaassen Z, Terris MK. Renal cell carcinoma: links and risks. Int J Nephrol Renovasc Dis. 2016;9:45-52.
-
Alhussaini AJ, Steele JD, Nabi G. Comparative Analysis for the Distinction of Chromophobe Renal Cell Carcinoma from Renal Oncocytoma in Computed Tomography Imaging Using Machine Learning Radiomics Analysis. Cancers (Basel). 2022;14(15):3609.
-
Dechet CB, Bostwick DG, Blute ML, Bryant SC, Zincke H. Renal oncocytoma: multifocality, bilateralism, metachronous tumor development and coexistent renal cell carcinoma. J Urol. 1999;162(1):40-2.
-
Lossos C, Ferrell A, Duncan R, Lossos IS. Association between non-Hodgkin lymphoma and renal cell carcinoma. Leuk Lymphoma. 2011;52(12):2254-61.
-
Abdel-Rahman O. Risk of Subsequent Primary Kidney Cancer After Another Malignancy: A Population-Based Study. Clin Genitourin Cancer. 2017;15(5):e747-e754.
-
Umer M, Mohib Y, Atif M, Nazim M. Skeletal metastasis in renal cell carcinoma: A review. Ann Med Surg (Lond). 2018 Jan 31:27:9-16.
-
Patchell RA, Tibbs PA, Regine WF, Payne R, Saris S, Kryscio RJ, Mohiuddin M, Young B. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. 2005;366(9486):643-8.
Articole din ediţiile anterioare
ONCOLOGICAL SURGERY | Ediţia 2 47 / 2019
Proteina C reactivă (PCR) şi leucocitele din lichidul peritoneal – rol în predicţia fistulelor digestive înalte
Virgiliu Mihail Prunoiu, Marian Augustin Marincaş, Tudor Marian Proca, Maria Manuela Răvaş, Eugen Bratucu
Fistulele anastomotice în chirurgia digestivă reprezintă o complicaţie gravă, care poate duce la decesul pacientului. Identificarea unor prob...
16 mai 2019
REVIEW | Ediţia 4 / 2015
Tratamentul paliativ şi suportiv în cancerul bronhopulmonar avansat
Alexandru Grigorescu
Lucrarea caută să prezinte concis aspecte esenţiale în terapia paliativă şi suportivă a cancerului bronhopulmonar avansat. Se face distincţia între...
24 noiembrie 2015
CASE PRESENTATION | Ediţia 1 / 2015
Tratamentul carcinomului renal metastatic cu terapiile TKI şi mTOR: prezentare de caz
Conf. dr. Dana Lucia Stănculeanu, Daniela Zob, Andreea Lăzescu
Lucrarea de faţă descrie medicamentele disponibile la ora actuală pentru tratamentul cancerului renal avansat. Acestea sunt reprezentate de mai m...
24 martie 2015
RADIOTERAPIA METASTAZELOR | Ediţia 1 / 2016
Rolul radioterapiei în managementul metastazelor osoase
Berna Akkus Yildirim, Yurday Ozdemir, Erkan Topkan
Metastazele osoase (MO) sunt întâlnite la unu din doi pacienți oncologici, de la prezentare sau pe parcursul evoluției bolii. Ca o regulă fundament...
24 martie 2017