High blood pressure in children represents a clinical syndrome which appears when the value of arterial tension is over the 95th percentile for age, weight and sex. It is a global health issue, doubling the risk of heart diseases and it is the third risk factor for mortality and morbidity in the world. Taking into consideration that the origin of hypertension was in childhood, our study proposes a detailed analysis from a clinical and biological point of view, on a retrospective study of hypertension cases registered in the Department of Pediatric Cardiology of the “Sf. Maria” Emergency Clinical Hospital for Children, Iaşi, from January 2015 to January 2018.
CLINICAL STUDIES
Hipertensiunea arterială la copilul de azi – începutul unei boli cronice la adultul de mâine
High blood pressure in today’s child – the beginning of a chronic disease in tomorrow’s adult life
Alina-Costina Luca,
Cătălina Luca,
Alexandra Luca,
Elena Ţarcă,
Bogdan A. Stana,
Mădălina Mardare,
Heidrun Adumitrăchioaiei
First published: 16 martie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Pedi.61.1.2021.4717
Abstract
Rezumat
Hipertensiunea arterială la copil reprezintă un sindrom clinic care apare atunci când valoarea tensiunii arteriale depăşeşte percentila 95 pentru vârstă, greutate şi sex. Este o problemă publică de sănătate la nivel mondial, dublând riscul apariţiei bolilor de inimă. Este al treilea factor de risc pentru mortalitate şi morbiditate în lume. Luând în considerare faptul că originea hipertensiunii arteriale a fost în copilărie, studiul nostru retrospectiv propune o analiză detaliată a cazurilor de hipertensiune arterială la copil internate în Clinica de cardiologie pediatrică a Spitalului Clinic de Urgenţă pentru Copii „Sf. Maria”, Iaşi, din ianuarie 2015 până în ianuarie 2018.
Introduction
High blood pressure is currently a global health issue, being the main controllable risk factor for cardiovascular and cerebrovascular diseases, but at the same time, the most difficult to manage in terms of therapy, hypertension, a noninfectious pandemic, affecting more than 40% of the US population, being a major factor in increasing cardiovascular morbidity and mortality.
The diagnosis of high blood pressure is currently made when the value of systolic or diastolic blood pressure is higher than the 95th percentile for age, sex and height in the age group 1-12 years old and higher than 130/89 mmHg for those older than 13 years old(2).
Stage I of hypertension falls within blood pressure values above the 95th percentile and up to 5 mmHg above the 99th percentile, while stage II represents more than 5 mmHg above the 99th percentile.
The definition of prehypertension in pediatrics is given by that value of systolic or diastolic blood pressure higher or equal to the 90th percentile but less than the 95th percentile. The average of three measurements performed at an interval of 5 minutes represents the value of the blood pressure.
The global prevalence of hypertension was estimated in 2015 at 1.3 billion, while in Central and Eastern Europe the prevalence exceeded 150 million cases.
With a prevalence in children between 1% and 5%, in healthy newborns the prevalence is 0.2%; the data look different when we refer to the newborn (premature or term) hospitalized in intensive care units, where the percentage is between 1% and 2.5%, the main causes being renal: renovascular disease and renal parenchymal diseases, followed by cardiovascular pathologies, endocrine pathologies and history of umbilical catheterization(1).
In teenagers, the prevalence of high blood pressure reaches 13%(1). This increase in percentage with age is associated with excess weight, which is why there is an underestimation of the prevalence due to the increase in the number of pediatric people affected by obesity(2).
High blood pressure in pediatric patients has been associated with left ventricular hypertrophy, increased carotid intima and cognitive impairment(3).
The National High Blood Pressure Education Program Working Group recommends hypertension screening starting at the age of 3 years old for all children, except for those at high risk for high blood pressure (premature, low birth weight, congenital cardiovascular disease, kidney disease), where the screening is recommended before 3 years old.
The appearance of signs and symptoms indicates a moderate/severe hypertension, which is most often of secondary cause, where the basic pathology also gives us the specific clinical and paraclinical picture. In newborns, difficulty eating, tachypnea without a known cause, apnea, irritability or lethargy are possible causes of hypertension. The 95th percentile for sex, age and height leads us to the diagnosis of hypertension. Often asymptomatic, it is diagnosed in routine medical checkups.
Materials and method
We performed a retrospective study on a group of 7517 children and adolescents hospitalized in the Department of Pediatric Cardiology of the “Sf. Maria” Emergency Clinical Hospital for Children, Iaşi, between January 2015 and January 2018.
We determined the value of blood pressure by the auscultatory method, with the child at rest, in a sitting position, with the right arm positioned at the level of the heart. Blood pressure was determined three times for each case, the validation value being represented by the average of the three determinations. We introduced in the study those patients whose average falled within the definition of prehypertension and hypertension.
The aim of the study was to evaluate patients with hypertension from a clinical and biological point of view. Data obtained during the anamnesis: presence of hereditary-collateral history of hypertension, the age when the disease began, comorbidities, the etiology of hypertension, presence of signs and symptoms announcing the occurrence of hypertensive complications, effects on growth and weight, paraclinical investigations, and therapy performed before hospitalization. The clinical and interclinical evaluations performed consisted in the examination of the cardiovascular system, the nutritionist evaluation in order to establish the growth-weight development, and the ophthalmologist also performed the fundus examination, in order to establish a possible endocrine cause – pheochromocytoma, hyperaldosteronism or hypercorticism, and the patients benefited from an endocrinological consultation. The etiology of epistaxis was detected by ENT consultation, the assessment of mental status was performed by the pediatric neuropsychiatrist and, last but not least, the geneticist evaluated the suspected cases of genetic abnormalities associated with hypertension.
There were performed the determination of complete blood count, the evaluation of inflammatory syndrome (leukocyte formula, leukocyte count, ESR, PCR), the evaluation of iron metabolism, urinalysis and urine culture, serum electrolytes, macroelements, serum urea, thyroid function tests, the evaluation of liver function – ALAT, ASAT, LDH, bilirubin, bile acids, alkaline phosphatase. It was also performed the holter monitoring during 24 hours, in order to establish episodes of hypertension, white coat hypertension, to establish the diagnosis of hypertension, HTAS, transient hypertension, prehypertension and grade I hypertension. Furthermore, there were performed: electrocardiogram, evaluation of heart performance by echocardiography, abdominal, renal and endocrine gland ultrasound in order to detect incriminated pathologies in the production of high blood pressure values, chest X-ray to evaluate the aorta, highlighting left ventricular hypertrophy. All these explorations were proposed and performed in the vast majority of cases of the entire group of 277 pediatric patients.
Results
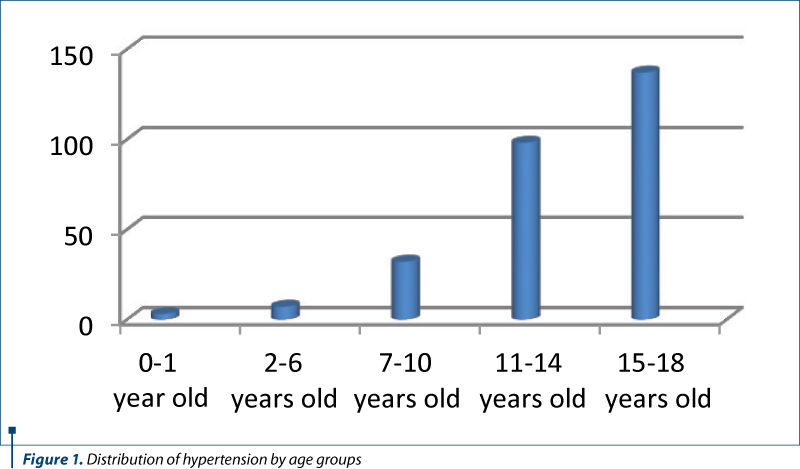
Age-related increases in blood pressure have been observed, the fewest cases being recorded in newborns, in early childhood and in middle-aged children. In the age range 0-10 years old, there were 42 cases; between 11 and 14 years old, there were 98 patients hospitalized during the study, and the rest of the group (137 cases, about half of the total of 277 cases) were between 15 and 18 years old.
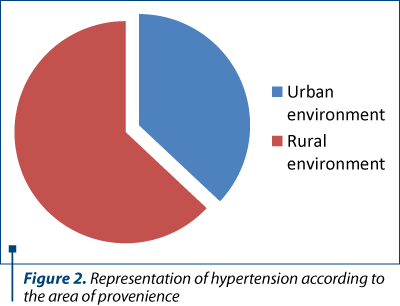
It is important to know the percentages depending on the environmental factors. To prevent better, we analyzed the study group from this point of view and we obtained a preponderance in rural areas (63%).
The analysis according to sex highlighted a slight difference between the two sexes, the highest percentage being in males (150 cases were registered, out of the 277 introduced in the study).
Analyzing the patients in terms of age and sex, in the age group 0-11 years old, 33 were males and 21 were females. In the age group 12-18 years old, 118 patients were boys and 105 were girls. In both age groups, males were found in higher percentages, which was also evident in the analysis of cases by sex. Males had higher percentages if we analyze the distribution according to the environment of origin and by sex.
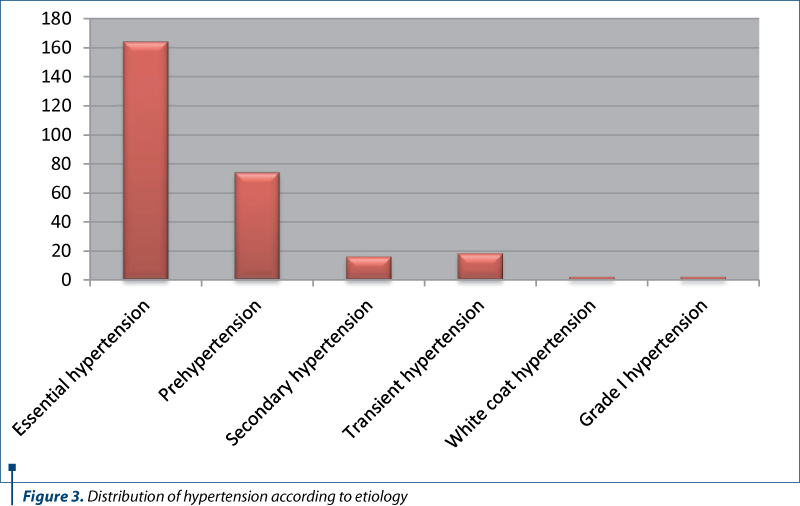
Essential hypertension was incriminated in a number of 167 cases, out of 277, which represents 59%, in contradiction with the literature, where it appears in percentages of 10-15%. In the first years, the presence of essential hypertension is increased, which is supported by data from literature. In this study, the increased percentage of those with essential hypertension is explained by the large number of patients aged 12-18 years old, the age at which hypertension can set in.
Prehypertension, the situation in which, if intervened effectively, hypertension can be avoided in the long run, was registered in 74 cases (26%), while secondary hypertension was registered in 16 cases (6%). Transient hypertension was found in 18 cases, accounting for 7%.
Obesity is constantly growing, becoming a global health problem, and it is often associated with hypertension. That’s why we evaluated the group according to Body Mass Index: 18% were overweight and only one child of the total was diagnosed with stature-weight hypotrophy. We wanted to find out the type of hypertension in the 51 patients diagnosed with overweight, and we found out that 55% of them had essential hypertension, 24% had prehypertension, 12% had secondary hypertension, 4% had transient hypertension, and 5% had grade I hypertension.
Heredity is a factor involved in the onset of hypertension, 84% of all parents mentioning that they had no cardiovascular disease, a significant percentage, which leads us to think either of a young age of parents (and, for this reason, the symptoms did not set in), or the lack of attention to oneself. The hypertension present in both parents was registered in a small percentage (1%), maternal hypertension was present in 7% of cases, and paternal hypertension was present in 6%.
The genetic damage was established, following the interclinical consultation, by the geneticist, in 16 cases: one case with Turner syndrome, cubitus valgus, MASS phenotype and pectus excavatum, two cases with café-au-lait spots and Down syndrome, and five cases with craniofacial dysmorphia, out of which two patients had hypertension, two were with hasty hypertension and one with transient hypertension. Down syndrome, Turner syndrome, pituitary dwarfism, MASS phenotype, pectus excavatum, cubitus valgus and patients with café-au-lait spots also showed essential hypertension.
In the case of antihypertensive patients, the electrocardiographic examination may reveal normal trajectory, changes in left/right ventricular hypertrophy, changes in the ST segment and in the T wave.
Of the total number of patients, in 240 cases the electrocardiography could be performed, in the rest of the cases the lack of cooperation led to the appearance of the artifacts, canceling the ECG. Of the 240 patients examined, 14% had QT prolongation, 10% had T-wave changes, minor right ram block was registered in 5%, ventricular overload was noticed in 1% of cases, and HVS was also present in 1%, the remaining 67% showing a normal electrocardiographic route.
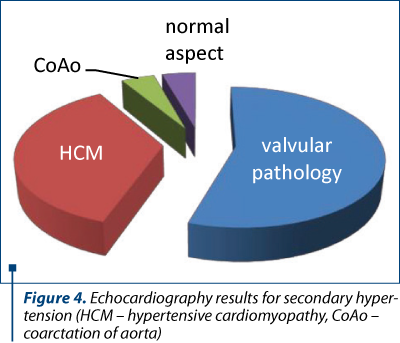
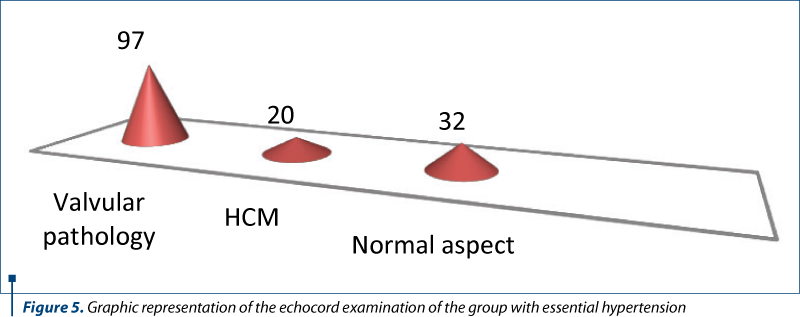
Echocardiography was performed on 149 children, and it showed the presence of valvular pathologies in 65% of cases – mitral regurgitation, tricuspid regurgitation, mitral valve prolapse, aortic insufficiency, 13% had changes in hypertrophic cardiomyopathy and only 22% had a normal echocord examination.
It should be noted that in the cases with transient hypertension, valvular pathology and hyperkinetic heart syndrome had a percentage of 61%, followed by hypertrophic cardiomyopathy, and only 6% had a normal echo heart appearance. In the case of prehypertension or borderline blood pressure, the positions remained approximately the same as in the transient hypertension.
The group of those with secondary hypertension included a number of 16 cases, and the valvular pathology had, again, a significant percentage, followed by hypertrophic cardiomyopathy and aortic coarctation.
The cardiological examination also included holter monitoring, which was possible in 51 cases. After monitoring, 18% of cases had transient hypertension, 22% had prehypertension and 60% had inconclusive results; out of this percentage, which represented 31 cases, 11 children were with unsystematized extrasystolic arrhythmia with a tendency to systematize, a case with blood pressure values at the upper limit, a hypertensive episode and the rest up to 31 had normal blood pressure values.
The ophthalmological evaluation did not reveal any case of hypertensive retinopathy, out of the 55 patients who benefited from this examination.
Hygienic-dietary treatment together with the recommendation of therapy for hypocalcemia, iron deficiency anemia and hypomagnesaemia were instituted in approximately 86% of cases. Monotherapy with antihypertensive drugs was introduced in 11% of cases and 6 patients required double antihypertensive therapy.
Discussion
The statistical analysis of the group showed that in the age group 15-18 years hypertension was found in a percentage of 49%, while in infants it appeared in 1% of cases. The prevalence of hypertension in the newborn and infant in our study overlaps with the results from most studies. A study conducted in Australia on 2600 newborns over a 4-year period showed a prevalence of hypertension of 1.3%. In numerous studies, also highlighted by the present study, the main cause incriminated in the increase in hypertension in older children and adolescents is excess body weight.
From the total of 7517 patients introduced in the study, in the Department of Pediatric Cardiology of the “Sf. Maria” Emergency Clinical Hospital for Children, Iaşi, between 1.01.2015 and 1.01. 2019, a number of 277 presented prehypertension or hypertension. Expressed as a percentage, the number of those diagnosed with blood pressure values above the limit accepted as normal, represented 3.68%, a value that is included in the percentage of 1-5% obtained in all specialized studies conducted during the last years. A retrospective cohort study, on more than 1.2 million pediatric patients, from 27 states, published in Pediatrics (vol. 138, number 6, December 2016), revealed a percentage of 3.3% for those diagnosed with hypertension.
A study conducted in Central India by Goel and published in 2016, which randomly evaluated 1221 adolescents aged 14 to 17 years old, in the hospital environment, revealed that 10.45% had high blood pressure, a prevalence much higher than the one determined in our country and in most European countries.
This fact can be explained by the cultural, socioeconomic differences and the older age group of the study group.
In Italy, 4% of school children had high blood pressure, and of these, only 1-3% were children with normal body weight, 37% of those with high blood pressure being overweight or obese (new study).
Obesity is often associated with high blood pressure. Following our analysis of BMI, 50 of the 277 patients with high blood pressure also associated high levels of BMI, within the definition of obesity or overweight.
The environment is an important factor, the lack of information, the lack of specialized medical staff, the difficult access to high-performance medical services, the socioeconomic situation, often precarious, are factors that lead to the increase of those with high blood pressure.
The presence of essential hypertension was 59%, although the literature gives us 10-15% for the pediatric population in case of this form of hypertension. The new studies explain the increase in the percentage of essential hypertension by the increase in the number of obese patients and by the changes in the modern lifestyle, based almost exclusively on sedentarism.
The main changes at the echocord examination were represented by valvular pathology – mitral regurgitation, tricuspid regurgitation, mitral valve prolpals, hyperkinetic heart syndrome, followed by hypertrophic cardiomyopathy.
However, at the end of the investigations, analyzing each case, it was concluded that a percentage of approximately 86% of patients can reduce their blood pressure values using a hygienic-dietary regime. The presentation to the doctor, for most of them, was performed in time to avoid antihypertensive medication and organic lesions secondary to untreated hypertension. We can say that, in the conditions of maintaining a proper hygienic-dietary diet, the vast majority will achieve the prevention of hypertension. Reducing salt intake, weight loss for overweight or obese people, introducing a diet based on fruits and vegetables, regular exercise, stopping smoking and alcohol consumption, where appropriate, and reducing stress are parts of the hygienic-dietary treatment that can reduce blood pressure values and can prevent the initiation of the pharmacological treatment. Monotherapy was introduced in 11% of cases, double antihypertensive therapy in 2% of cases, and triple therapy in 1% of all those under drug therapy.
In the aforementioned study, a percentage of those placed under antihypertensive drug therapy of 5.6% was obtained, noting that the percentage is almost half of the percentage of those who received medication in our study. This higher number can be explained by the fact that the lack of medical information present in our country, the lack of periodic checkups at the general practitioner office, and the lack of medical staff, especially in rural areas, lead to cases of pediatric hypertension that require a much higher number of cases to introduce medication than in other countries.
This high percentage should draw our attention to the introduction of screening controls, educating parents and children about the benefits of breastfeeding, diversification, consumption of fruits and vegetables and constant physical effort.
The main classes of antihypertensives used are angiotensin converting enzyme inhibitors, angiotensin 2 receptor blockers, followed by diuretics, calcium channel blockers and the latest beta-blockers.
Conclusions
With an underestimated prevalence especially due to the lack of determination of blood pressure values during each medical visit, in an era of sedentary lifestyle and excessive eating, hypertension in children is more common, those pediatric patients often becoming adults with high blood pressure. This major public health issue, hypertension, the leading cause of cardiovascular risk events, affects more than 1 billion people worldwide.
Increasing the number of pediatric studies, training medical staff in schools and in general practitioners offices in order to measure blood pressure efficiently and regularly, educating the population on the major risk of high blood pressure, introducing national programs to identify children at risk of developing high blood pressure are some means by which we can prevent the increase in the number of children with hypertension, as well as limiting the number of hypertensive adults.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
- Iordache C. Pediatrics, 1st ed. “Gr. T. Popa” Publishing House, UMF Iaşi, 2011.
- Anton DA, Deacon G, Gregory I, Oltean C, Rose ML. Pediatrics – fundamentals. “Gr. T. Popa” Publishing House, UMF Iaşi, 2012.
- Baciu A. Essential Arterial Hypertension occuring in Children and Teenagers. Anthropological Correlations. International Journal of Collaborative Research on Internal Medicine and Public Health. 2012;4(6):1017-1039.
Articole din ediţiile anterioare
STUDII CLINICE | Ediţia 4 / 2016
Evaluarea nutriţională cu particularităţi evolutive la pacienţii cu mucoviscidoză
Prof. dr. Evelina Moraru, Ramona Diaconu, Aurica Rugină
Mucoviscidoza este cea mai frecventă maladie monogenică, autozomal recesivă, în populațiile de origine caucaziană, cu evoluție cronică, letală, cu ...
09 noiembrie 2016
GHID | Ediţia 1 / 2015
Recomandări actuale în managementul şi urmărirea astmului bronşic la copil
Bogdan A. Stana
Astmul bronşic reprezintă cea mai frecventă boală cronică a copilăriei şi principala cauză de morbiditate, având drept consecinţe absenteism şcolar...
12 martie 2015
STUDII CLINICE | Ediţia 2 50 / 2018
Sindromul hiper-IgE − între provocări clinice şi complexitate patogenică
Prof. dr. Evelina Moraru, Ionuţ Albu
Sindromul hiper-IgE este o imunodeficienţă primară complexă, ce implică sistemul imun, oasele, ţesutul conjunctiv şi dinţii. Alături de valorile m...
29 mai 2018
STUDII CLINICE | Ediţia 4 48 / 2017
Intervenţii nutriţionale precoce în dislipidemii la vârsta pediatrică și riscul pentru sindrom metabolic
Bogdan A. Stana, Giorgiana Bran, Dan Moraru, Alice Azoicăi
Tulburările metabolismului lipidic reprezintă o patologie relativ frecventă la vârsta pediatrică, existând două etiologii principale: terenul ge...
09 ianuarie 2018