Integrative psychiatry seeks to link to the biological perspective various factors with a role in the prophylaxis and treatment of severe mental disorders (SMD). In the context of stigmatization of SMD patients, a sad reality promoted by the media, starting from events in which aggressive and violent behaviors come to the forefront of public attention, it is necessary to find risk factors with predictive value for such behaviors, as a preliminary stage of initiating policies for prophylaxis, early detection and treatment in SMD. Clinical, neurobiological and genetic factors are explored in this work, which is based on the analysis of data from literature, but also on our own studies, with the aim of integrating, in an approach with both theoretical and practical implications, the data necessary to create strategies to prevent violent behaviors in patients with SMD. Factors such as extrapyramidal phenomena, hypoglycemia, alcohol abuse, brain trauma, elevated C-reactive protein values, personal history of ADHD or conduct disorder, mitochondrial dysfunction, and genetic and epigenetic risk factors are all assessed for their contribution to the onset of aggressive behaviors in schizophrenia. It is expected that future research will confirm the predictive value of at least some of these factors, so that the next stage may begin – i.e., the finding of prophylactic and therapeutic strategies.
The concept of integrative psychiatry and the assessment of risk factors of antisocial potential in patients with schizophrenia
Conceptul de psihiatrie integrativă şi evaluarea factorilor de risc ai potenţialului antisocial la pacienţii cu schizofrenie
First published: 23 aprilie 2024
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Psih.76.1.2024.9461
Abstract
Rezumat
Psihiatria integrativă urmăreşte asocierea la perspectiva biologică a unor factori complementari cu rol în profilaxia şi tratamentul tulburărilor mintale severe (TMS). În contextul în care stigmatizarea pacienţilor cu TMS este o realitate promovată mediatic, pornind de la evenimente în care comportamentele agresive şi violente ajung în prim-planul atenţiei publice, este necesară găsirea factorilor de risc cu valoare predictivă pentru astfel de comportamente, ca etapă preliminară a iniţierii unor politici de profilaxie, detecţie precoce şi tratament în TMS. Factorii clinici, neurobiologici şi genetici sunt exploraţi în această lucrare, care se bazează pe analiza datelor din literatură, dar şi pe studii proprii, cu scopul de a integra, într-un demers cu implicaţii atât teoretice, cât şi practice, datele necesare compunerii unei strategii de prevenţie a comportamentelor violente la pacienţii cu TMS. Elemente precum fenomenele extrapiramidale, hipoglicemia, consumul abuziv de alcol, traumele cerebrale, valori crescute ale proteinei C reactive, istoricul personal de ADHD sau de tulburare de conduită, disfuncţiile mitocondriale, factorii de risc genetici şi epigenetici, toate sunt evaluate din perspectiva contribuţiei la apariţia comportamentelor agresive în schizofrenie. Este de aşteptat ca viitoarele cercetări să confirme valoarea predictivă cel puţin a unora dintre aceşti factori, astfel încât să se poată trece la următoarea etapă, cu rol profilactic şi terapeutic.
Introduction
The concept of complementary and integrative psychiatry brings into discussion a multidimensional perspective on the neurocognitive component of severe psychiatric disorders (SPD) and appeals to the possibilities of using into the current practice pharmacological therapies combined with nonpharmacological alternatives or complementary modalities of intervention. These interventions refer in particular to the lifestyle factors and the possibility of their sanogenetic modification, including the application of healthy nutrition-oriented programs.
Unlike allopathic medicine and psychiatry, which focus their fundamental scientific research activity on detecting genetic vulnerability factors, complementary and integrative medicine aims to identify and control epigenetic factors that contribute to the pathogenesis of schizophrenia and other SPD(1,2). DNA hypermethylation and hypomethylation have been associated with schizophrenia in studies exploring post-mortem brain tissues and peripheral blood markers(3). Other epigenetic findings suggest that changes in the non-coding RNAs, especially microRNAs and long-chain non-coding RNAs, have been explored in schizophrenia as potential predictors of treatment response(3). Data on histone modification in patients with schizophrenia is still in the early phases of research, but future studies are expected to bring new insights into this field of epigenetics(3,4). Drugs triggering epigenetic modifications are also expected to be more intensively researched, due to their pragmatical importance – for example, valproic acid, which can inhibit histone deacetylases (HDACs) and induce DNA demethylation(4). HDAC2 functions involve the modulation of synaptic plasticity, learning and memory(4).
Genetic and epigenetic alterations may be translated into biochemical signatures, detected through metabolomics-oriented investigations(5). Gut microbiota alterations have also been involved in the pathophysiology of aggressive behavior(5). Therefore, interventions targeting gut microbiota modification may be of interest for managing psychotic symptoms, although research in this field is still beginning to emerge(6,7). Complementary and integrative medicine is focused exactly on such nonpharmacological interventions aimed at producing biological effects compared to prescribed medications(6).
This article explores data in the literature regarding the potential predictors of aggressive and violent behavior in schizophrenia and also presents new, unpublished data on patients diagnosed with schizophrenia, retrospectively analyzed in a forensic context. The objectives are both theoretical – i.e., to determine the clinical, genetic and neurobiological factors with a potential predictive role for violent behaviors in schizophrenia spectrum disorders, but also pragmatical, because these risk factors should be integrated into any program focused on prophylaxis, therapy, and de-stigmatization of patients with these disorders.
Core dimensions of integrative psychiatry applied in the research of schizophrenia
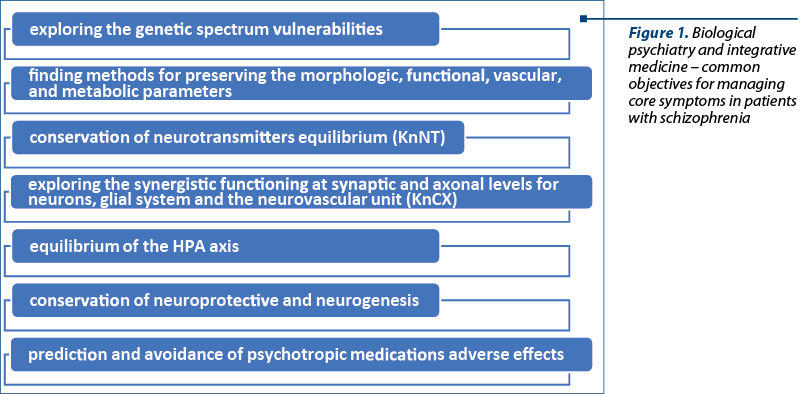
From the perspective of biological psychiatry and clinical psychopharmacology, the concept of integrative medicine, in our opinion, pursues several goals: (1) integration of genetic vulnerability risk factors in a more complex context – i.e., “the genetic spectrum vulnerabilities”; (2) finding the adequate methods for preserving optimal cerebral morphologic, functional, vascular and metabolic parameters; (3) conservation of the neurotransmitters equilibrium and neurotransmission constant (KnNT)(8,9); (4) exploring the substrate of synergistic functioning at synaptic and axonal levels for neurons, glial system and the neurovascular unit, with a focus on preserving the connectivity constant (KnCX)(8,9); (5) maintaining the equilibrium of the hypothalamic-pituitary-adrenal (HPA) axis; (6) conservation of the neuroprotective and neurogenesis capacity; (7) prediction and avoidance of adverse effects induced by psychotropic medication, depending on genetic and epigenetic vulnerabilities (Figure 1).
In the category of genetic risk factors, the DISC1 (Disrupted-in-Schizophrenia 1) gene has been correlated with decreased hippocampal volume and an increased risk for ventriculomegaly(10). In animal models, DISC1 disruption negatively affects presynaptic and postsynaptic dopaminergic function, leading to increased locomotion after amphetamine administration, higher dopamine levels after amphetamine injection in the nucleus accumbens, and irregular basal dopamine levels, dopamine receptor levels, and binding potentials(11).
The previously mentioned cerebral structural changes that appear in relation to the DISC1 gene were correlated with the clinical observations of Huber and Gross’s longitudinal studies of patients with schizophrenia(12). These structural changes were considered significant markers predicting the risk of negative evolution and major cognitive deficits in schizophrenia(13). Ventriculomegaly causes the subventricular granular area to decrease to the point of disappearance, and this area is of extreme importance due to its role in substitutive neurogenesis at the hippocampal level, a mechanism that explains the progressive cognitive deterioration of schizophrenia in patients with DISC1 genetic defect. In animal studies, the DISC1 gene was correlated with a cellular disturbance – i.e., impairment of the cytoskeletal protein activities(14,15).
Neuregulin 1 (NRG1) is a pleiotropic growth factor responsible for changes in the efficiency of neural connectivity and development(16). Disruption of the NRG1 gene has a negative impact on the neurodevelopmental processes and the restorative neurogenetic mechanisms, favoring the occurrence of synaptic dysconnectivity (synaptopathy), axonal dysfunctions (axonopathy), but also impairments of the neurovascular unit, the neuron-astroglia ratio and the GAP-junction and TIGH-junction, favoring neurodegeneration(16-18). NRG1 has an important role in glutamatergic signaling through N-methyl-D-aspartate (NMDA) receptors, which explains its role in synaptic plasticity(16-18). Altered isoforms of NRG1, especially type I and type IV, have been associated with schizophrenia or with risk alleles(16). The altered expression of erbB3, one of the NRG1 receptors, has occurred in the prefrontal cortex of patients with schizophrenia, suggesting the involvement of this growth factor in the pathogenesis of chronic psychoses(18).
Genetic alteration of vascular growth factors can cause capillary-type vascular irrigation dysfunctions, abnormalities that cause vascular hypoperfusion at the level of neuronal or glial structures(19,20). This, in turn, favors neuronal apoptosis or causes angiopathy within the white matter, which can be aggravated by hypoxic hyperglutamatergic encephalopathy of the newborn and which causes changes within the structure of the periventricular white matter, the so-called “periventricular leukomalacia”(19). This epigenetic mechanism, added to the DISC1 genetic vulnerability, may be involved in triggering multisystemic risk mechanisms involved in the development of schizophrenia.
The aforementioned genetic mechanisms can be assembled in a “spectrum of genetic vulnerabilities”. The most representative of this spectrum are genetic vulnerability for Parkinson’s disease and genetic vulnerabilities for conditions determined by mitochondrial dysfunction(21-25). Extrapyramidal effects observed in patients with schizophrenia after the administration of antipsychotic medications have been significantly associated with aggressive behaviors in the primary analysis(21). The aggressive group had more severe akathisia, but the difference was not significant(21). The association between the confirmed genetic mechanisms and the complementary ones can be synergistic, becoming an aggravating factor in the evolution of schizophrenia. Failure to control akathisia can lead to suicidal ideation, aggression and violence(22). Withdrawal akathisia may occur when the dose of antipsychotic medication is decreased or the drugs are discontinued(22). Aggression in Parkinson’s disease and related disorders with a dopaminergic pathophysiology has a high incidence and prevalence, and this is an understudied dimension of the neurological disease(23).
Following this line of reasoning, the recognition of complementary genetic mechanisms allows for the facilitation of prophylaxis mechanisms destined to mitigate the dysfunctions caused by the synergistic association. Such a phenomenon could significantly improve the evolution and prognosis of schizophrenia spectrum disorders.
Aggressive behaviors in schizophrenia
We believe that aggressivity, manifested in acts of hetero- and self-aggressive violence, is the main manifestation of patients with schizophrenia responsible for the social stigmatization of these individuals, because such behaviors are heavily publicized and have a major emotional impact on the general population. This type of antisocial behavior has a multifactorial, biological and psychosocial determinism and can be triggered by environmental factors or unfavorable interrelational contexts.
Biological psychiatry, by identifying neurobiological and genetic vulnerability factors, may significantly contribute to the prediction of the risk of such aggressive-violent manifestations and can support the research for preventive measures. Such measures involve effective psychosocial or pharmacological intervention, applied in crisis situations.
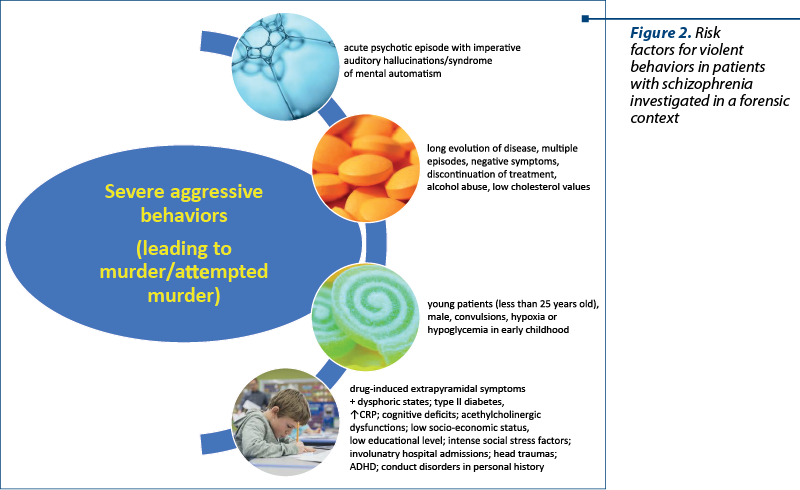
From the studies carried out by the collective of the Discipline of Psychiatry within the University of Medicine and Pharmacy of Craiova, studies coordinated by Univ. Prof. T. Udriştoiu (PhD) and Univ. Prof. D. Marinescu (PhD) on a group of patients diagnosed with schizophrenia, paranoid type, who associated violent behavior, leading to murder or attempted murder, the following clinical-pharmacological risk factors were identified (Figure 2):
-
Acute psychotic episode with imperative auditory hallucinations or syndrome of mental automatism.
-
Patients with a long evolution of the disease and multiple psychotic episodes, predominant negative symptoms of medium or severe intensity, accompanied by discontinuation of the pharmacological treatment, consumption of alcohol or psychoactive substances, and low values of the cholesterol level.
-
Young patients, aged below 25 years old, male, with acute onset of psychosis and the presence of imperative auditory hallucinations, who had in their early childhood febrile convulsions and hypoxia or hypoglycemic crises at birth.
-
Patients with multiple episodes, with drug-induced extrapyramidal syndromes, such as parkinsonism or akathisia, accompanied by dysphoric states.
-
The presence of obesity and type 2 diabetes mellitus (probably drug-induced, against the background of a spectrum genetic vulnerability) and accompanied by an increase in proinflammatory factors (C-reactive protein).
-
Cognitive deficit, important to be assessed by neuropsychological examinations and dysfunctions of the acetylcholinergic system, possibly favored by the use of antipsychotic medication with anticholinergic effect or corrective antiparkinsonian medication, with the same anticholinergic effect.
-
Patients with low socioeconomic status, low educational level, and a history of repeated forensic events.
-
The existence of intense social stress factors, objectified by repeated involuntary hospital admissions.
-
The presence of head trauma in the personal history and the use of illicit drugs, as well as the identification in the personal history, during childhood and adolescence, of social, physical and verbal abuse; attention deficit hyperactivity disorder (ADHD) and impulsive-explosive conduct disorders, but also depression with suicidal ideation and early alcohol consumption (type 1 and 2 Cloninger) were identified in the personal history of these patients. It is worth mentioning that childhood conduct disorder has previously been reported as a potential contributor to schizophrenia due to the failure to learn not to behave aggressively in early life, impairments in understanding emotional faces, maltreatment and re-victimization(26). Specific genetic variants related to stress regulation in combination with adversity have been associated with aggressive behaviors and psychotic symptoms(26). An efficient treatment of conduct disorder and prevention of re-victimization may help reduce the risk of aggressive behaviors in schizophrenia(26).
From the biological psychiatry perspective, aggressivity and violence in schizophrenia are associated with the disconnective type of functional imbalance between the cortical system and the limbic system. At the cortical level, a reduction in serotonin levels was reported, with excessive compensatory increases in dopamine and norepinephrine neurotransmission(27). This aspect explains the psychotic onset dominated by productive, hallucinatory-delusional phenomena, accompanied by psychomotor agitation, but also the existence of a high potential for triggering impulsive behaviors and episodes of depression, with the risk of impulsive suicidal behaviors.
At the cerebral level, neuroimaging studies have highlighted, in patients with schizophrenia and violent behavior, the existence of lesions and disconnectivity of the orbitofrontal cortex with the amygdala, the anterior cingulate cortex, and the hippocampus(28). Hippocampal dysfunction is associated with genetic vulnerability, altered substitutive neurogenesis, and connectivity between the frontal cortex and limbic system(28,29).
The progressive hippocampal lesion causes a marked alteration of cognition and, through the disconnective mechanisms at the limbic system, amygdala and frontal cortex, it diminishes the inhibitory cognitive control over impulsive behavior activation(28,29).
The existence of cerebral microlesions correlated with neurodevelopmental abnormalities in patients with schizophrenia and diabetes mellitus can be explained by recurrent episodes of hypoglycemia(30). Hypoglycemia may thus trigger violent and aggressive behaviors, in the presence of a vulnerable neurobiological terrain, with the loss of behavioral control and the onset of antisocial manifestations(30). Hypoglycemia can also be triggered secondary to alcohol consumption, the dual pathology of schizophrenia-alcoholism being a major risk factor for the onset of violent behaviors(30-32). Mild traumatic brain injuries and alcohol abuse are important risk factors for aggressive and violent behaviors, therefore treating adequately comorbid substance use disorders is essential for preventing further negative evolution in patients with schizophrenia and comorbid misuse of addictive substances(32-35).
Conclusions
Based on the reviewed data, we believe that the integrative perspective applied in the field of biological psychiatry may highlight a series of clinical, genetic and biological predictive factors for aggressivity and violence in schizophrenia. If such factors are validated by further research, then a prediction of aggressive behaviors would be possible in this vulnerable population and the risk of violence could be diminished by applying a correct prophylactic approach.
In the context of mass media-promoted stigmatization of patients with psychiatric disorders, mitigating the violence and aggression in schizophrenia through prophylactic and therapeutic interventions is an important objective for mental health specialists. If reached, this objective could be decisive in the social reintegration of patients with chronic psychotic disorders. Controling for extrapyramidal symptoms, hypoglycemia and mitochondrial dysfunction may reduce the risk of violent behavior in individuals with schizophrenia.
Corresponding author: Ileana Marinescu E-mail: marinescu_psy@yahoo.com
CONFLICT OF INTEREST: none declared.
financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY.

Bibliografie
-
Nguyen SA, Oughli HA, Lavretsky H. Complementary and integrative medicine for neurocognitive disorders and caregiver health. Curr Psychiatry Rep. 2022;24(9):469-480.
-
Nguyen SA, Lavretsky H. Emerging complementary and integrative therapies for geriatric mental health. Curr Treat Options Psychiatry. 2020;7(4):447-470.
-
Chen Q, Li D, Jin W, Shi Y, Li Z, Ma P, et al. Research progress on the correlation between epigenetics and schizophrenia. Front Neurosci. 2021;15:688727.
-
Peedicayil J. Epigenetic management of major psychosis. Clin Epigenetics. 2011;2(2):249-256.
-
Manchia M, Fanos V. Targeting aggression in severe mental illness: The predictive role of genetic, epigenetic, and metabolomic markers. Prog Neuropsychopharmacol Biol Psychiatry. 2017;77:32-41.
-
Vasiliu O. Is fecal microbiota transplantation a useful therapeutic intervention for psychiatric disorders? A narrative review of clinical and preclinical evidence. Curr Med Res Opin. 2023;39(1):161-177.
-
Varteresian T, Lavretsky H. Complementarity and integrative therapy in psychiatry. Focus (Am Psychiatr Publ). 2018;16(1):54-56.
-
Marinescu I, Udriştoiu I, Marinescu D. Choroid plexus calcification: clinical, neuroimaging and histopathological correlations in schizophrenia. Rom J Morphol Embryol. 2013;54(2):365-369.
-
Marinescu I, Predescu A, Udriştoiu T, Marinescu D. Comparative study of neuroprotective effect of tricyclics vs. trazodone on animal model of depressive disorder. Romanian Journal of Morphology and Embryology. 2012;53(2):397-400.
-
Ochneva A, Zorkina Y, Abramova O, Pavlova O, Ushkova Vmorozova A, et al. Protein misfolding and aggregation in the brain: Common pathogenetic pathways in neurodegenerative and mental disorders. Int J Mol Sci. 2022;23(22):14498.
-
Dahoun T, Trossbach SV, Brandon NJ, Korth C, Howes OD. The impact of Disrupted-in-Schizophrenia 1 (DISC1) on the dopaminergic system: a systematic review. Transl Psychiatry. 2017;7:e1015.
-
Huber G, Gross G. The concept of basic symptoms in schizophrenic and schizoaffective psychoses. Recenti Prog Med. 1989;80(12):646-52.
-
Huber G, Gross G. The development of the psychopathology in Germany in the last decades. Psychiatria Biologica. 1995;3:65-72.
-
Ozeki Y, Tomoda T, Kleiderlein J, Kamiya A, Bord L, Fujii K, et al. Disrupted-in-schizophrenia-1 (DISC-1): Mutant truncation prevents binding to NudE-loke (NUDEL) and inhibits neurite outgrowth. Proc Natl Acad Sci USA. 2003;100(1):289-294.
-
Lipska BK, Mitkus SN, Mathew SV, Fatula R, Hyde TM, Weinberger DR, Kleinman JE. Functional genomics in postmortem human brain: abnormalities in a DISC1 molecular pathway in schizophrenia. Dialogues Clin Neurosci. 2006;8(3):353-357.
-
Law PJ, Law AJ. Neuregulin 1 and schizophrenia: genetics, gene expression, and neurobiology. Biol Psychiatry. 2006;60(2):132-140.
-
Stefansson H, Steinthorsdottir V, Thorgeirsson TE, Gulcher JR, Stefansson K. Neuregulin 1 and schizophrenia. Ann Med. 2004;36(1):62-71.
-
Corfas G, Roy K, Buxbaum JD. Neuregulin 1-erbB signaling and the molecular/cellular basis of schizophrenia. Nat Neurosci. 2004;7(6):575-80.
-
Gilmore JH, Castillo M, Rojas M. Early onset schizophrenia in a patient with premature birth, germinal matrix hemorrhage and periventricular leukomalacia. Schizophr Res. 2000;44(2):158-60.
-
Thomas KL, Huttunen M. Neural migration, pro-inflammatory interleukins and periventricular leukomalacia: involvement in schizophrenia. Trends Neurosci. 1999;22(9):389-90.
-
Cheung P, Schweitzer I, Crowley KC, Yastrubetskaya O, Tuckwell V. Aggressive behaviour and extrapyramidal side effects of neuroleptics in schizophrenia. Int Clin Psychopharmacol. 1996;11(4):237-40.
-
Lipinski JF Jr, Mallya G, Zimmerman P, Pope HG Jr. Fluoxetine-induced akathisia: clinical and theoretical implications. J Clin Psychiatry. 1989;50(9):339-42.
-
Macchi ZA, Miyasaki J, Katz M, Galifianakis N, Sillau S, Kluger BM. Prevalence and cumulative incidence of caregiver-reported aggression in advanced Parkinson disease and related disorders. Neurol Clin Pract. 2021;11(6):e826-833.
-
Rajesekaran A, Venkatasubramanian G, Berk M, Debnath M. Mitochondrial dysfunction in schizophrenia: pathways, mechanisms and implications. Neurosci Biobehav Res. 2015;48:10-21.
-
Roberts RC. Mitochondrial dysfunction in schizophrenia: With a focus on postmortem studies. Mitochondrion. 2021;56:91-101.
-
Hidgins S. Aggressive behavior among persons with schizophrenia and those who are developing schizophrenia: Attempting to understand the limited evidence on causality. Schizophr Bull. 2017;43(5):1021-1026.
-
Brisch R, Saniotis A, Wolf R, Bielau H, Bernstein HG, Steiner J, et al. The role of dopamine in schizophrenia from a neurobiological and evolutionary perspective: Old fashioned, but still in vogue. Front Psychiatry. 2014;5:47.
-
Hoptman MJ, D’Angelo D, Catalano D, Mauro CJ, Shehzad ZE, Kelly AMC, et al. Amygdalofrontal functional disconnectivity and aggression in schizophrenia. Schizophr Bull. 2010;36(5):1020-1028.
-
Curcic-Blake B, Nanetti L, van der Meer L, Cerliani L, Renken R, et al. Not on speaking terms: hallucinations and structural network disconnectivity in schizophrenia. Brain Struct Funct. 2015;220:407-18.
-
Shukla AP, Dickison M, Coughlin N, Karan A, Mauer E, Truong W, et al. The impact of food order on postprandial glycaemic excursions in prediabetes. Diabetes Obes Metab. 2019;21(2):377-381.
-
De Angelis LC, Brigati G, Polleri G, Malova M, Parodi A, Minghetti D, et al. Neonatal hypoglycemia and brain vulnerability. Front Endocrinol (Lausanne). 2021;12:634305.
-
Vasiliu O. Therapeutic management of schizophrenia and substance use disorders dual diagnosis - clinical vignettes. RJMM. 2018;CXXI(2):26-34.
-
Stovicek PO, Friedmann C, Marinescu D, et al. Mild TBI in the elderly - risk factor for rapid cognitive impairment in Alzheimer’s disease. Rom J Morphol Embryol. 2020;61(1):61-72.
-
Vasiliu O, Vasile D, Făinărea AF, et al. Analysis of risk factors for antipsychotic-resistant schizophrenia in young patients - a retrospective analysis. RJMM. 2018;CXXI(1):25-29.
-
Fritz M, Soravia SM, Dudeck M, Malli L, Fakhoury M. Neurobiology of aggression - Review of recent findings and relationship with alcohol and trauma. Biology (Basel). 2023;12(3):469.
Articole din ediţiile anterioare
Tratamentul farmacologic în schizofrenie
Ghidurile de tratament oferă recomandări bazate pe dovezi pentru a-i asista pe practicieni în situații clinice specifice. Ele reprezintă un instrum...
Analiza transnosografică a disfuncţiei executive – dimensiuni clinice, psihometrice şi terapeutice
Analiza disfuncţiei executive la pacienţii cu tulburări psihice prezintă interes din punct de vedere clinic şi terapeutic, având în vedere cercetăr...
Tulburările psihotice în ICD-11 comparativ cu ICD-10
Capitolul privitor la psihoze din ICD-11 prezintă modificări semnificative în raport cu ICD-10, începând cu plasarea în ordinea prezentării tulbură...
Delir religios la un pacient schizofren cu traseu EEG de tip iritativ în lobul temporal stâng
Schizofrenia este o tulburare psihiatrică ce este caracterizată prin simptome pozitive (delir şi halucinaţii), simptome negative (aplatizare afecti...