The pregnant woman’s diet must be varied and balanced; the deficiency of some nutrients can have serious repercussions on the development of the fetus and on the health of the newborn. Omega-3 essential fatty acids are some of the most important nutrients for both the health of the pregnant woman and the newborn. This work aims to discuss current data on omega-3 essential fatty acid (PUFA) deficiency during pregnancy and lactation, as well as the possible long-term risks to the fetus and baby. Most experts recommend eating fish and seafood as the main source of omega-3 in the context of a healthful diet and regular physical activity. The beneficial effects of omega-3 essential fatty acids during pregnancy and lactation have been confirmed by a large number of clinical trials. The results of the studies were in agreement on the association of EPA/DHA with the favorable evolution of pregnancy. Enriching the diet with omega-3, before and during pregnancy, can have beneficial effects for both mother and fetus. According to EFSA (2009), an amount of 120-340 mg of omega-3 per day is sufficient before and during pregnancy, for the beneficial effects of the cardiovascular, ocular and central nervous system. Omega-3 fatty acids ensure the development of the brain and contribute to the formation of the fetal retina and the normal psychomotor development of the fetus. Still, a sufficient intake of omega-3 fatty acids during pregnancy decreases the risk of preeclampsia, combats postnatal depression, and reduces the risk of preterm birth. The symptoms of omega-3 fatty acid deficiency during pregnancy were highlighted in children at different ages until the age of 6-8 years old: poorer results in verbal and IQ performance tests, and poorer results of communication skills and abilities.
Actualităţi privind deficitul de acizi graşi esenţiali omega-3 în sarcină şi riscurile asupra fătului
New insights regarding the deficiency of omega-3 essential fatty acids in pregnancy and the risks to the fetus
First published: 17 noiembrie 2021
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Gine.34.4.2021.5696
Abstract
Rezumat
Alimentaţia gravidei trebuie să fie variată şi echilibrată, deficitul unor nutrienţi putând avea repercusiuni grave asupra dezvoltării fătului şi a stării de sănătate a nou-născutului. Acizii graşi esenţiali omega-3 sunt unii dintre cei mai importanţi nutrienţi atât pentru sănătatea gravidei, cât şi pentru cea a nou-născutului. Această lucrare îşi propune să aducă în discuţie datele actuale privind deficitul acizilor graşi esenţiali (PUFA) omega-3 în perioada sarcinii şi alăptării, cât şi posibilele riscuri asupra fătului şi a copilui pe termen lung. Majoritatea experţilor recomandă consumul de peşte şi fructe de mare ca sursă principală de omega-3, în contextul unei alimentaţii sănătoase şi al unei activităţi fizice regulate. Efectele benefice ale acizilor graşi esenţiali omega-3, în timpul sarcinii şi alăptării, au fost confirmate într-un număr foarte mare de studii clinice. Rezultatele studiilor sunt în consens în ceea ce priveşte asocierea EPA/DHA cu evoluţia favorabilă a sarcinii. Îmbogăţirea alimentaţiei cu omega-3 înainte şi în timpul sarcinii poate avea efecte benefice atât pentru mamă, cât şi pentru făt. Conform EFSA (2009), o cantitate de 120-340 mg de omega-3 pe zi (cu o medie de 250 mg de omega-3 pe zi) este suficientă înainte şi în timpul sarcinii, pentru efectele benefice cardiovasculare, oculare şi asupra sistemului nervos central. Acizii graşi omega-3 asigură dezvoltarea creierului şi contribuie la formarea retinei fătului şi la dezvoltarea psihomotorie normală a acestuia. Totodată, un aport suficient de acizi graşi omega-3 în timpul sarcinii scade riscul apariţiei preeclampsiei, combate depresia postnatală şi reduce riscul apariţiei naşterii premature. Simptomele deficitului de omega-3 în timpul sarcinii au fost evidenţiate la copii la vârste diferite, până la vârsta de 6-8 ani: rezultate mai slabe la testele verbale şi privind coeficientul de inteligenţă, rezultate mai slabe ale competenţelor şi abilităţilor de comunicare.
Introduction
Pregnancy and breastfeeding are very important periods in a woman’s life. Healthy eating during pregnancy is more important than ever. Every woman has a different body and different nutritional needs, but during pregnancy and lactation every woman must consume a diet that includes a variety of foods, in small and regular meals, to provide all the nutrients she needs. The diet of pregnant women must also provide them with the nutrients necessary for the proper development of the fetus.
Omega-3 are essential fatty acids that should be consumed in our diet. The human body can synthesize many other fatty acids, such as saturated and monounsaturated fatty acids, but it cannot synthesize fatty acids with the first double bond to omega-3 and omega-6. Essential fatty acids, omega-3 and omega-6, are lipids that cannot be synthesized in the body and must be ingested through diet or dietary supplements(1).
The current recommendations for the daily diet of pregnant women and during breastfeeding are: 2-3 servings of legumes, 1-2 servings of fish, 1-2 servings of chicken/turkey, one serving of red meat. The pregnant woman is recommended to consume at least 120 to 340 g of fish per week if at least one serving is fatty fish (herring, mackerel, sardines, salmon, catfish etc.), which are good sources of omega-3 essential fatty acids(2).
Polyunsaturated fatty acids act as precursor molecules for eicosanoids. They regulate fundamental physiological processes (division and growth cell, hormonal secretions and cell membrane transport activity)(3).
Omega-3 polyunsaturated fatty acids belong to the family of polyunsaturated fatty acids (PUFA) with a long chain of carbon atoms and are represented by alpha-linoleic acid (ALA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA). Alpha linoleic acid is considered essential because it cannot be synthesized by the body, the main source of food being food. ALA can be transformed in human tissues to EPA and DHA, but the amounts are not significant (less than 5%)(2).
Alpha-linolenic acid (ALA) is found in vegetable fats – in high concentrations in flax seeds, rape, nuts and soybeans. In general, plants contain ALA and not EPA or DHA. Eicosapentaenoic acid and docosahexaenoic acid are found in fish fat. Most experts recommend eating fish and seafood as a source of omega-3 in the context of a healthy diet, along with regular physical activity(1,4).
Depending on the fat content, we distinguish between species of lean fish (cod, pikeperch, perch and hake) and fatty fish (herring, mackerel, sardines, salmon and catfish). EPA is found in abundance in fatty fish (tuna, salmon, herring and cod liver) and in marine animal oil. All forms of fish and seafood contain omega-3. Fatty fish contains a higher amount of omega-3 compared to lean fish(4).
The increased intake of EPA and DHA in the body is considered to be improved by the constant consumption of oil from cold-water fish and krill. Crude fish oil contains 18% EPA and 12% DHA; by special processing, it can be concentrated, obtaining oil with 33% EPA and 22% DHA. Another essential source of omega-3 fatty acids is currently seaweed (Crypthecodinium cohnii and Schizochytrium microalgae)(5).
Materials and method
The aim of our research is to highlight the recommendation of consumption of essential polyunsaturated fatty acids omega-3 during pregnancy and lactation and to present the results of the monitoring of children whose mothers received or not optimal amounts of omega-3 during pregnancy, at different intervals until the age of 8 years old.
In order to achieve our objectives, we looked for clinical trials collected from three databases: Cochrane Pregnancy and Childbirth’s Trials Register, ClinicalTrials.gov and WHO International Clinical Trials Registry Platform (ICTRP) (August 16, 2020) and from prospective longitudinal studies. Using the keywords “omega-3” OR “polyunsaturated fatty acids” AND “pregnancy” OR “gestation”, we selected randomized controlled trials (RCTs) which compared the group that included women who were given omega-3 fatty acids during pregnancy (in the form of supplements or foods, either on their own or with a co-intervention) with the group who received placebo or lacked omega-3 administration. Children were evaluated after birth at different time intervals, and the results of different groups were compared.
Results and discussion
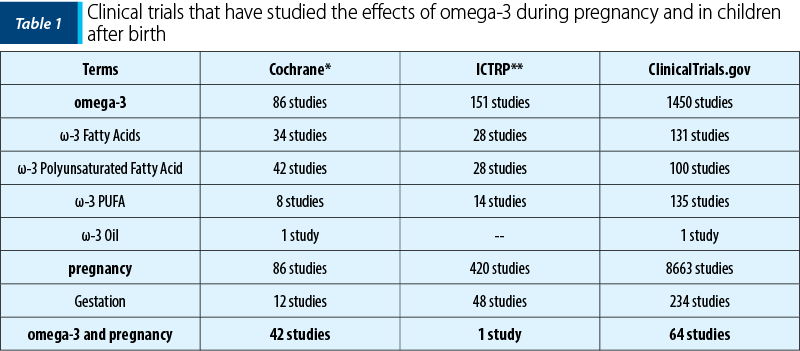
We found a number of 107 studies conducted between 2007 and 2020 that met the established search criteria, with over 2400 articles that published the results of these studies. The number of randomized controlled trials in the three databases is specified in Table 1.
What are the recommended doses
of omega-3 polyunsaturated fatty acids
in pregnancy and lactation?
For optimizing results during pregnancy and for the health of the fetus, the guidelines recommend that the pregnant woman consume at least 200 mg of DHA per day. A pregnant woman can achieve this threshold by consuming one to two servings of seafood per week(6).
Fruits may also contain organic mercury and other harmful toxins (e.g., polychlorinated biphenyls; PCBs), which could be harmful to the fetus during growth. For this reason, the FDA/EPA recommends limiting the consumption of fish to two servings (approximately 340 g of seafood) per week(6-9).
According to the European Food Safety Authority (2012), an amount of 250 mg of omega-3 per day is sufficient as consumption, before and during pregnancy, for the beneficial effects on the pregnant woman and the fetus(10).
Recent studies have shown that, despite the FDA/EPA opinion, which recommends up to 2 servings of fish as safe in pregnancy, many pregnant women consume little or no fish during this period, thus depriving the fetus of the necessary nutrients. Pregnant women indicated that the advice of a doctor played a key role in their decision to eat fish during pregnancy(11).
What are the effects of consuming omega-3 polyunsaturated fatty acids on the fetus and mother during pregnancy?
Numerous benefits have been associated with the consumption of omega-3 polyunsaturated fatty acids during pregnancy or after birth when fish or seafood are found in the diet. Polyunsaturated fatty acids (PUFAs) are necessary for the body’s physiological functions, including oxygen transport, energy storage, cell membrane function, regulation of inflammation and cell proliferation, but also for the growth and the development of many systems and organs during pregnancy, the most important being the brain and the eye(7,8,12-14).
The preponderance of the data suggests that the intake of omega-3 polyunsaturated fatty acids during pregnancy is important for the development of the fetal brain and for the subsequent neurodevelopment of the baby. Fetal brain growth accelerates in the second half of pregnancy, and the growth rate remains high in the infant in the first year and continues to grow for the next few years. Dietary deprivation of omega-3 polyunsaturated fatty acids in pregnancy is associated with impaired development and behaviour(12-15).
In a longitudinal prospective study – Avon Longitudinal Study of Parents and Children (ALSPAC) – that recruited 13,761 pregnant women, they were asked to complete opinion polls on seafood consumption during pregnancy and to answer questions about their children’s development and behavior. A number of 10,000 children were evaluated at six months, one year and a half (18 months), two years and a half (30 months), three years and a half (42 months) and six years and a half (81 months) and at eight years. The respondents were grouped according to their seafood consumption into several study groups: no seafood consumption, 1 to 340 g per week, and more than 340 g per week consumption(16).
Mothers who ate more than 340 g of seafood per week had children who did not show poorer results in verbal and IQ performance tests than children born of mothers who ate less than 340 g per week of seafood. Children born to mothers who did not report any seafood intake during pregnancy had the highest risk of side effects or suboptimal test results, with the lowest quartile for verbal test and IQ performance at 8 years of age, behavioral problems at 7 years of age and poor early development scores on tests to assess fine motor skills, social behaviors, skills and communication skills. For those women who ate seafood during pregnancy and in whom seafood consumption was higher, it was found that the likelihood of having the baby results below the optimal level was reduced(16-19).
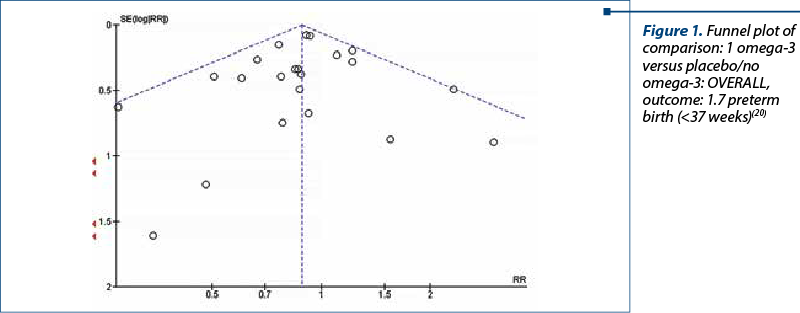
Increasing the intake of omega-3 during pregnancy, either through supplements or in food, may reduce the incidence of premature birth (before 37 weeks and before 34 weeks; Figure 1) and may lead to a less likelihood of having a child small at birth. Women who take omega-3 supplements during pregnancy may also be more likely to have longer pregnancies(20,21).
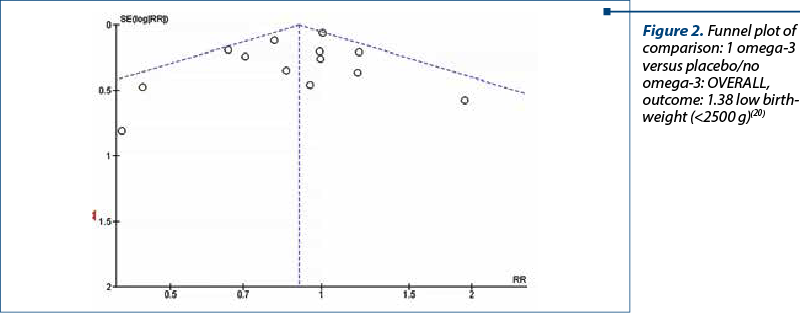
The rates of low birth weight (below 2500 g) showed a 10% relative risk reduction with omega‐3 LCPUFA compared with no omega‐3 (RR 0.90; 95% CI; 0.82 to 0.99; 15 trials, 8449 participants) – Figure 2. No obvious asymmetry was observed on visual assessment of a funnel plot for this outcome(20,21).
The meta-analysis included 40 randomized controlled trials (RCTs; this type of study provides the most reliable results, and involved 19,927 women), conducted mostly in middle- or high-income countries, and evaluated both high-risk women, the risk of preterm birth, as well as women without this risk. One group of pregnant women received omega-3 LCPUFA (long-chain polyunsaturated fatty acids) and, in studies, they were compared with another group of women who received placebo (they thought they were receiving omega-3 LCPUFA, but it was a placebo) or with another group of women who did not receive omega-3 LCPUFA at all(12,13).
The quality of evidence in the included studies ranged from high to very low; this determined the certainty of the findings for different results. The incidence of premature birth (before 37 weeks) and very premature birth (before 34 weeks) was found to decrease in women who received omega-3 LCPUFA compared to women who did not receive additional omega-3. There were also fewer low-birth-weight babies. However, omega-3 LCPUFA probably increased the incidence of pregnancies that continued over 42 weeks(17-19).
Recent studies have shown that the intake of omega-3 fatty acids seems to be important during breastfeeding. Women who were breastfeeding and who received 200 mg of DHA per day in their diet for four months had infants who had significantly better results on the Bayley Psychomotor Development Index tests performed after 30 months, compared with women who received a vegetable oil supplement(12,15).
Fish oil supplements are given during pregnancy, and lactation also leads to a lower risk of allergies in infants(22). During the first 12 months of monitoring, children born from mothers who received omega-3 had a decreased risk of developing food allergies and IgE-associated eczema.
The implications of omega-3 on mothers’ health showed that a sufficient intake during pregnancy decreases the risk of preeclampsia and combats postnatal depression among mothers(23,24). Other symptoms of omega-3 fatty acid deficiency in the mother include extreme fatigue, memory impairment, dry skin, changes in mood to depression and cardiovascular disorders(25,26).
Conclusions
The results of the clinical studies confirm the association of an optimal intake of EPA/DHA with the favorable evolution of pregnancy. An enriching diet with omega-3, before and during pregnancy, can have beneficial effects for both mother and fetus. According to EFSA (2012), an amount of 120 to 340 mg of omega-3 per day (medium: 250 mg of omega-3 per day) is sufficient before and during pregnancy for the beneficial effects of the cardiovascular, ocular and central nervous system.
Omega-3 fatty acids ensure the development of the brain, the nervous system and the formation of the fetal retina and contribute to the normal psychomotor development of the fetus and to the normal growth in the uterine cavity. Concurrently, a sufficient intake of omega-3 fatty acids during pregnancy decreases the risk of preeclampsia, combats postnatal depression and reduces the risk of premature birth.
Conflicts of interests: The authors declare no conflict of interests.
Bibliografie
Kominiarek MA, Rajan P. Nutrition Recommendations in pregnancy and lactation. Med Clin North Am. 2016;100(6):1199–215.
Bazinet RP, Laye S. Polyunsaturated fatty acids and their metabolites in brain function and disease. Nat Rev Neurosci. 2014;15(12):771–85.
Tur JA, Bibiloni MM, Sureda A, Pons A. Dietary sources of omega 3 fatty acids: public health risks and benefits. Brit J Nutr. 2021;107(Suppl 2):S23–S52.
Barta DG, Coman V, Vodnar DC. Microalgae as sources of omega-3 polyunsaturated fatty acids: Biotechnological aspects. Algal Research. 2021;58:102410.
Akerele OA, Cheema SK. A balance of omega-3 and omega-6 polyunsaturated fatty acids is important in pregnancy. J Nutr Intermed Metab. 2016;5:23-33.
Coletta JM, Bell SJ, Roman AS. Omega-3 fatty acids and pregnancy. Rev Obstet Gynecol. 2010;3(4):163-171.
Campoy C, Escolano-Margarit V, Anjos T, et al. Omega 3 fatty acids on child growth, visual acuity and neurodevelopment. Brit J Nutr. 2012;107:S85–S106.
Hidaka BH, Thodosoff JM, Kerling EH, Hull HR, Colombo J, Carlson SE. Intrauterine DHA exposure and child body composition at 5 y: exploratory analysis of a randomized controlled trial of prenatal DHA supplementation. Am J Clin Nutr. 2018;107(1):35‐42.
EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific opinion related to the tolerable upper intake level of eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA) and docosapentaenoic acid (DPA). EFSA J. 2012;10(7):2815.
Li G, Chen H, Zhang W, et al. Effects of maternal omega-3 fatty acids supplementation during pregnancy/lactation on body composition of the offspring: A systematic review and meta-analysis. Clin Nutr. 2018;37:1462-73.
Bernardi JR, de Souza Escobar R, Ferreira CF, Pelufo Silveira P. Fetal and neonatal levels of Omega-3: effects on neurodevelopment, nutrition, and growth. Scientific World Journal. 2012;2012:202473.
Birch EE, Garfield S, Castaneda Y, et al. Visual acuity and cognitive outcomes at 4 years of age in a double-blind, randomized trial of long chain polyunsaturated fatty acid-supplemented infant formula. Early Hum Dev. 2007;83(5):279-84.
Bosaeus M, Hussain A, Karlsson T, Andersson L, Hulthén L, Svelander C, et al. A randomized longitudinal dietary intervention study during pregnancy: effects on fish intake, phospholipids, and body composition. Nutr J. 2015 Jan 2;14:1.
Bergmann RL, Bergmann KE, Richter R, Haschke‐Becher E, Henrich W, Dudenhausen JW. Does docosahexaenoic acid (DHA) status in pregnancy have any impact on postnatal growth? Six‐year follow‐up of a prospective randomized double‐blind monocenter study on low‐dose DHA supplements. J Perinat Med. 2012;40(6):677‐84.
Fraser A, Macdonald-Wallis C, Tilling C, et al. Cohort Profile: The Avon Longitudinal Study of Parents and Children: ALSPAC mothers cohort. Int J Epidemiol. 2013;42(1):97–110.
Olsen SF, Halldorsson TI, Thorne-Lyman AL, et al. Plasma concentrations of long chain N-3 fatty acids in early and mid-pregnancy and risk of early preterm birth. EBioMedicine. 2018;35:325-33.
Shireman T, Kerling EH, Gajewski BJ, Colombo J, Carlson SE. Docosahexaenoic acid supplementation (DHA) and the return on investment for pregnancy outcomes. Prostaglandins Leukot Essent Fatty Acids. 2016;111:8‐10.
Scholtz SA, Kerling EH, Shaddy DJ, Li S, Thodosoff JM, Colombo J, et al. Docosahexaenoic acid (DHA) supplementation in pregnancy differentially modulates arachidonic acid and DHA status across FADS genotypes in pregnancy. Prostaglandins, Leukot Essent Fatty Acids. 2015;94:29-33.
Ali MK. The effect of omega 3 on pregnancy complicated by asymmetrical intrauterine growth restriction. Available at: https://clinicaltrials.gov/ct2/show/NCT02696577
Ali MK, Amin ME, Amin AF, Abd El, Aal DE. Evaluation of the effectiveness of low‐dose aspirin and omega 3 in treatment of asymmetrically intrauterine growth restriction: a randomized clinical trial. Eur J Obstet Gynecol Reprod Biol. 2017;210:231‐5.
Miles EA, Calder PC. Can early Omega-3 fatty acid exposure reduce risk of childhood allergic disease? Nutrients. 2017;9(7):784.
Wilson NA, Mantzioris E, Middleton PF, Muhlhausler BS. Influence of clinical characteristics on maternal DHA and other polyunsaturated fatty acid status in pregnancy: A systematic review. Prostaglandins Leukot Essent Fatty Acids. 2020;154:102063.
Cozma MA, Găman MA, Dobrică EC, Boroghină SC, Iancu MA, Creţoiu SM, Simionescu AA. A glimpse at the size of the fetal liver – is it connected with the evolution of gestational diabetes? Int J Mol Sci. 2021;222:7866.
Williams MA, Frederick IO, Qiu C, et al. Maternal erythrocyte omega-3 and omega-6 fatty acids, and plasma lipid concentrations, are associated with habitual dietary fish consumption in early pregnancy. Clin Biochem. 2006;39(11):1063–70.
Wieland LS, Santesso N. A summary of a Cochrane review: Omega-3 fatty acid addition during pregnancy. Eur J Integrative Med. 2019;27:131-132.
Articole din ediţiile anterioare
Copiii şi societatea modernă
În procesul devenirii şi desăvârşirii de sine, cuplul şi familia sunt calea, mijlocul şi şansa ca matrice fundamentală a vieţii. În şi prin familie...
Transmiterea materno-fetală a infecţiei HPV
Mai multe studii au analizat transmiterea materno-fetală a infecţiei cu virusul papiloma uman (HPV). Aceasta se poate realiza în perioada periconce...
Modificările statusului periodontal în sarcină – review şi prezentare a unui caz clinic
Sarcina este o perioadă caracterizată de schimbări fiziologice legate de o vulnerabilitate ridicată a sănătăţii orale. Variaţia prevalenţei modific...
Sarcina depăşită cronologic – riscuri şi management
În România, sarcina depăşită cronologic este definită ca o sarcină cu durată mai mare de 41 de săptămâni şi 0 zile. Determinarea unei sarcini...