In this paper, the importance of custom-fitted mouthguard is highlighted, because they are used in almost all specialties related to dentistry, including orthodontics and dental prosthetics, being used to solve as many problems as possible, such as: relaxing the TMJ muscles, correcting TMJ disorders, preserving and especially preserving the position of the teeth after orthodontic treatment, protection during performance sports, teeth whitening etc.
INTERDISCIPLINARY
Technological aspects in the manufacturing of custom-fitted mouthguard (Part I)
Aspecte tehnologice în confecţionarea gutierelor cu utilizare dentară (Partea I)
Ioana Voinescu,
Carmen-Georgiana Dorobanţu,
Radu Cătălin Costea,
Viorel Ştefan Perieanu,
Gabriela Tănase,
Mădălina Violeta Perieanu,
Mircea Popescu,
Bogdan Alexandru Dimitriu,
Irina Adriana Beuran,
Mihai Burlibaşa
First published: 24 noiembrie 2023
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/ORL.61.4.2023.8963
Abstract
Rezumat
În acest articol, am încercat să evidenţiem importanţa gutierelor dentare, deoarece acestea sunt utilizate în aproape toate specialităţile aferente stomatologiei, inclusiv în ortodonţie şi în protetica dentară, fiind întrebuinţate în rezolvarea cât mai multor probleme, cum ar fi: relaxarea musculaturii ATM, corectarea tulburărilor ATM, păstrarea şi mai ales conservarea poziţiei dinţilor după tratamentul ortodontic, protecţie în timpul practicării unui sport de performanţă, albirea dinţilor etc.
Introduction
Mouthguards are defined in specialized literature as a dental tool used for diagnosis and treatment, especially to alleviate the symptoms caused by temporomandibular disorders and bruxism(1-4).
But mouthguards in dentistry have multiple uses. They are used with great efficiency both in orthodontics and dento-facial orthopedics to preserve the therapeutic result, in prosthetic practice for the therapy of bruxism phenomena (it has the role of protection and repositioning of dental structures), and for performing teeth whitening procedures (supporting role for substances used for teeth whitening)(1-4). However, the main benefit of mouthguards is the fact that they balance the distribution of occlusal forces to all components of the masticatory system. They can reduce the frequency, but not the intensity, of parafunctional episodes and act for the prevention of complications determined in the masticatory system(1-4).
Thus, the situations in which the use of mouthguard is indicated are(1-5):
-
after orthodontic treatment;
-
for teeth whitening;
-
in the case of patients with bruxism;
-
for patients who practice various sports, especially contact sports;
-
within complex dental treatments, with a diagnostic role.
This article, structured in two distinct parts, presents several aspects that intervene in the technological flow of making mouthguards, using a sequence of very representative images.
Case presentation
1. Mouthguards used for teeth whitening (whitening trays)
A 24-year-old female patient presented to the dental office, wanting to perform a whitening of both dental arches, using a home whitening kit with whitening trays.
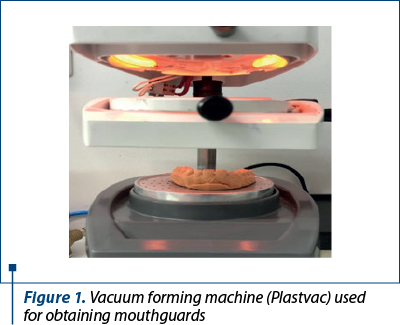
As materials and equipment used in the manufacture of whitening trays, the following should be mentioned: mouthguard laminates; the vacuum forming machine (Plastvac) (Figure 1); materials (type 3 and type 4 die stone, mixing bowl and spatula for mixing die stone, vibrating table); equipment and tools for processing and polishing (dental technique engine, burs, disc, fluff etc.); light-curing dental resin-based composites; special box for packaging and transport.
Mouthguard laminates are available in several variants, which differ in thickness, consistency or color. Their thickness varies between 1 and 5 mm. In general, depending on the type of mouthguard to be made, there are transparent or colored foils with various prints. Transparent foils are used to make professional mouthguards, while colored foils are used to make individualized mouthguards for athletes. For this case, a transparent mouthguard laminate of 1 mm thickness was chosen.
Carbide burs are used in the processing of mouthguards, which help to separate them from the mouthguard laminate after cooling. For cutting, you can also use the diamond cutter discs, taking care that the cutting path of the mouthguard is made in a straight line, because the inclination of the disc while rotating can break and cause accidents at the workplace.
Rubber wheels or points are used to finish the mouthguard and, at the end of the process, felt bobs wheel, cotton and cloth polishing brush can be used. The light-curing composite resin is used to create space for the gels intended for the actual whitening process in case of whitening trays. The composite material will be applied to the labial surface of the teeth and after the molding the mouthguard laminate on the model, that space intended for the whitening gels will be created. A special box is needed to transport the whitening tray and store it in good condition. The whitening tray will be placed in the box together with the instructions for use and storage for patients, and after that, the whole assembly can be sent to the dental office.
In the dental office, the dentist took the functional impressions of both dental arches of the patient with the help of two standard impression trays, using for the impression silicone condensation materials in double consistency (putty and light body) for maxillary arch and irreversible hydrocolloids for mandibular arch (Figure 2). Afterwards, the imprints were washed under running tap water for 20 seconds, then decontaminated by immersing them in chemical substances with disinfectant potential (substances based on quaternary ammonium salts), fully respecting the instructions recommended by the manufacturer.

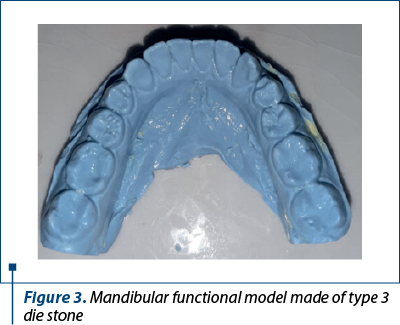
Next, the maxillary and mandibular functional models were made, by pouring type 3 die stone for mandibular model (Figure 3) and type 4 die stone for maxillary model.
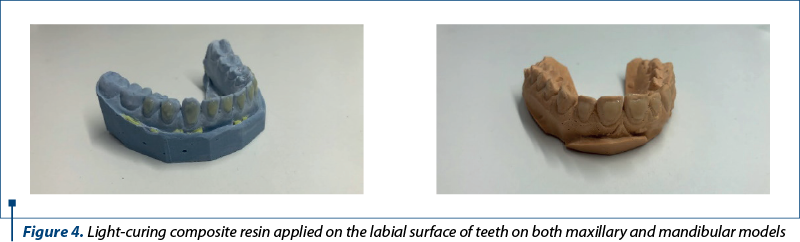
After trimming the models, light-curing composite resin is applied on the labial surfaces of all teeth, which has the role of creating space for the whitening gels. The composite material applied must not cover the teeth cervical line, and the amount of composite resin will not be exaggerated. This composite material was applied to both the upper functional model and the lower functional model (Figure 4).
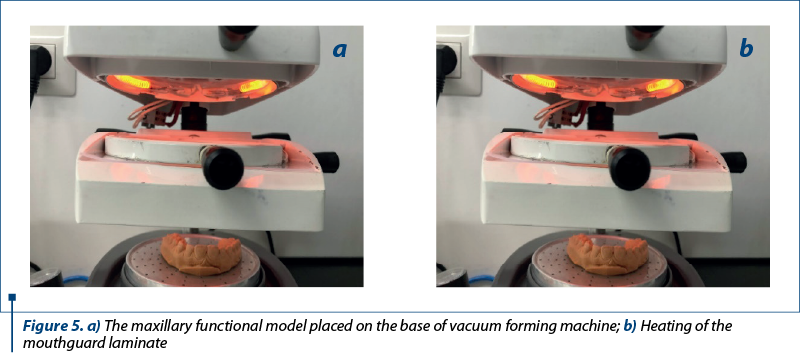
Each model will be positioned on the support in the middle of the vacuum forming machine and the mouthguard laminate is placed in the holding support near the heat source. The temperature at which the laminate will be heated can be set from the device system, a process that takes approximately 4-5 minutes when the machine is cold and 30-60 seconds when the machine is warm (Figure 5). With the help of the vacuum created by the forming machine, the foil will be applied, or more precisely molded on the functional model with very high precision, resulting in the actual mouthguard in a rough phase.
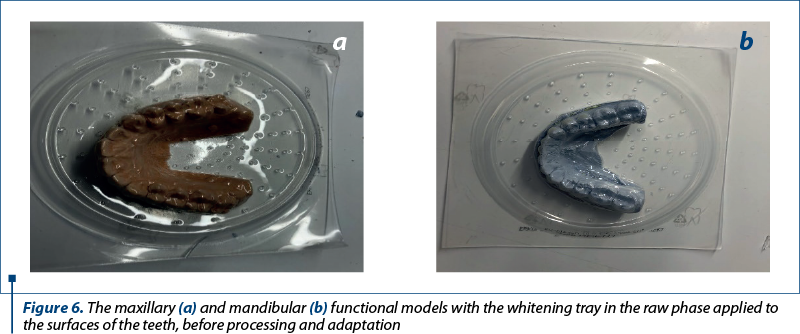
After the temperature of the laminate returns to normal, the processing of the mouthguard can begin (Figure 6).
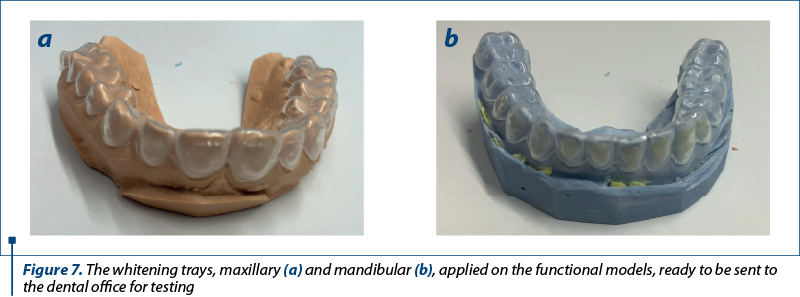
Using carbide burs or with the help of a diamond cutting disc, the remaining surplus of mouthguard laminate will be cut off, then the whitening tray will be processed as follows: on the labial and oral surface, the edge of the tray will follow the teeth cervical line, as close as possible. Practically, the aim is that the two whitening trays do not have sharp edges, the margins should be as rounded as possible. At the end, the tray will be polished, to be as smooth as possible, in order not to create discomfort for the patient (Figure 7).
After washing and disinfecting, the whitening trays will be placed in the special storage and transport box, together with recipes containing indications and way of keeping, and after a final checkup, they will be sent to the dental office (Figure 8). Once they arrive at the dental office, the dentist will try on the whitening trays in the patient’s oral cavity and check in detail whether they meet her requirements (Figure 9).


Also, in this first part of the article, some technological aspects will also be presented very briefly in terms of the manufacture of mouthguards for athletes, as well as night guards made of classic acrylic materials, the latter especially for patients with nocturnal bruxism. Sports and acrylic gutters have similar materials and work steps to those previously shown, with small specifications.
2. Mouthguards for athletes and sportsman
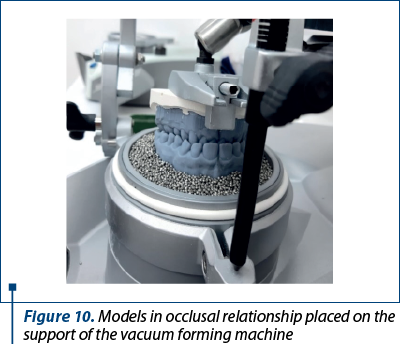
In order to create mouthguards for athletes and sportsman, it is necessary to take an impression of both dental arches, as well as to record the intermaxillary occlusal relationships, using a condensation silicone material of putty consistency. The dental technician will cast the two models, using type 3 die stone. The models placed in the occlusal relationship will be mounted on a special support of the vacuum forming machine (Figure 10).
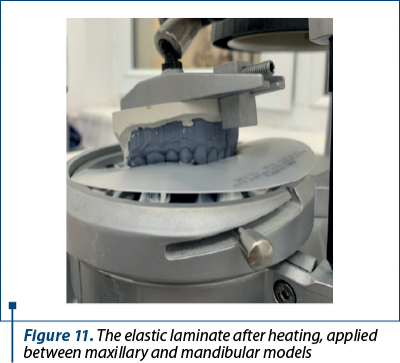
After lamination, the thermoplastic plate will be pressed on the maxillary model. It is actually a more special laminate in the case of mouthguards for athletes and sportsman, heaving different thickness, appearance and colors. After molding the laminate on the maxillary model, the mandibular model will be overlapped on the maxillary one, with another elastic mouthguard laminate placed between the two models (Figure 11). The role of this stage is to highlight the morphology of the teeth on the mouthguard made on the maxillary arch.
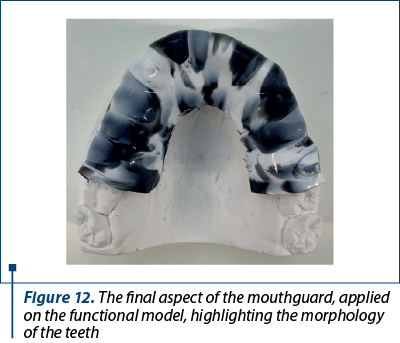
The mouthguard for athletes and sportsman must be processed, and its length should not completely cover the dental arches, but only partially (Figure 12). At the same time, this mouthguard will have on the occlusal surface a morphology of the lower teeth, but more erased, not very well highlighted.
3. Night guard – also known as bite guard, bite splint, occlusal guard or occlusal splint
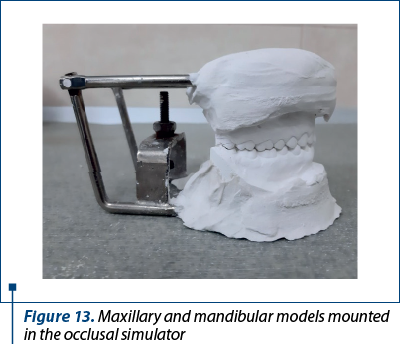
In the case of night guards, as in the case of mouthguards for athletes, it is necessary to take an impression of both dental arches, as well as to record the intermaxillary occlusal relationship. Both resulting functional models will be fitted in the occlusal simulator (Figure 13).
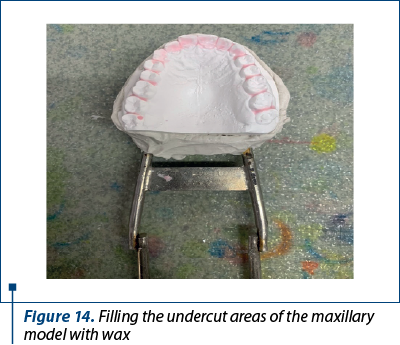
Because the acrylic resin acquires a degree of stiffness after the setting, to prevent the acrylate from entering the retentive areas of the dental arches, they are blocked using wax (Figure 14).
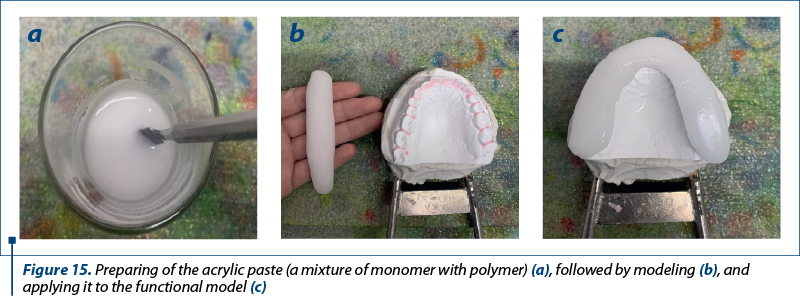
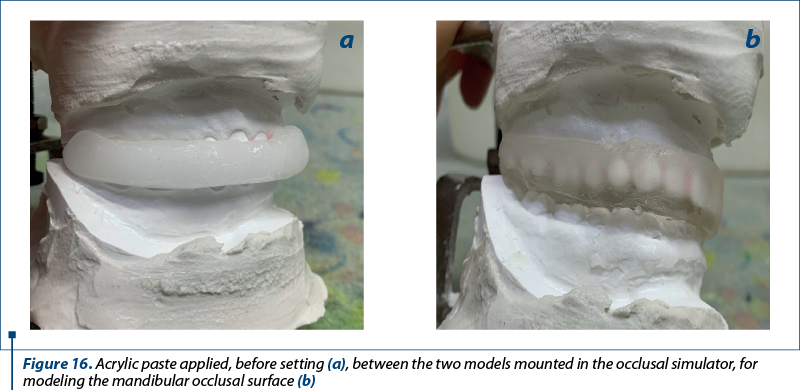
After mixing the powder and the liquid (the commercial form in which the acrylic resin is presented), from the moment it turns into a moldable paste, it is transformed into a roll and applied to the occlusal face of the teeth from the maxillary arch (Figure 15). Afterwards, the two models are brought together without making a firm contact between them, so a layer of acrylate remains between the two arches (Figure 16).
Discussion
Contrary to expectations, mouthguards were not first patented as dental devices. In 1949, William T. Oberto submitted a patent to the United States Patent office for a device entitled “Mandible cushion for oxygen masks”. It was patented a year later (5 September 1950) under the number 2,521,084(6), and it was a device designed to provide protection for the dental arches, tongue and lips, but at the same time allowing the patient to be oxygenated during convulsions that can appear in electric shock therapy(6,7).
Some years before this patent, several dentists referred to various devices used by boxers to preserve the integrity of the dental arches during boxing matches, among them A.M Abrams, W.H. Jacobs and J.W. Hagey(8-11). In fact, The National Alliance Football Rules Committee adopted a regulation in January 1962, requiring all highschool football players to wear dental guards(12). Thus, mouthguards were introduced for several categories of sports to prevent accidents at the level of the oral cavity and the teeth, in particular.
The appearance of new materials, such as dental ceramics, a brittle material that must be protected from parafunctions, but also thorough investigations related to TMJ dysfunction have led to the use of mouthguards (night guards) to protect the dental arches from parafunctions(13-15).
Mouthwashes experienced a new stage of evolution in 1989, when the widespread use of 10 percent carbamide peroxide for at-home teeth whitening began(16). Custom-fitted mouthguards (whitening trays) were made, provided with space for the application of the whitening substance, mouthguards that were to be used by patients during the night(17-19).
Conclusions
In this first part of the article, the importance was highlighted, but also the description of several technological aspects was carried out in the manufacture of dental mouthguards used for teeth whitening (whitening trays), for the protection of teeth by athletes (mouthguards) and classic acrylic night guards for patients with nocturnal bruxism.
Practically, the manufacturing of mouthguards is not at all expensive in terms of equipment and consumables, it is not a complex process, and can be done in a relatively short time. It should also be highlighted that the patient must be very well informed about how to use and store the mouthguards.
Acknowledgement: Viorel Ştefan Perieanu and Gabriela Tănase are corresponding authors (Viorel Ştefan Perieanu: viorelperieanu@yahoo.com; Gabriela Tănase: tanasegabriela2@gmail.com); Bogdan Alexandru Dimitriu and Irina Adriana Beuran have equally contribution with the first author.
Conflict of interest: none declared.
Financial support: none declared.
This work is permanently accessible online free of charge and published under the CC-BY licence.

Bibliografie
-
Cristache CM, Bunea I, Şelaru EP. Albirea dentară între mit şi realitate - Scurt review. Dental Target. 2016;11(38):10-16.
-
Lavigne GJ, Khoury S, Abe S, Yamaguchi T, Raphael K. Bruxism physiology and pathology: an overview for clinicians. J Oral Rehabil. 2008;35(7):476-94.
-
Ojovan A, Burlacu V, Cartaleanu A, Cuşnir A, Bălan E. Optimizarea alegerii tratamentului în hipersensibilitatea ţesuturilor dure ale dintelui. Medicina Stomatologică. 2010;16(3):62-64.
-
Frazier KB, Haywood VB. Teaching nightguard bleaching and other tooth-whitening procedures in North American dental schools. J Dent Educ. 2000;64(5):357-64.
-
Oancea L, Manolache T. Realizarea gutierei ocluzale prin tehnologia CAD-CAM. Dental Target. 2015;10(4):30-35.
-
Patents Google. Mandible cushion for oxygen masks US2521084A [cited 19.02.2023]. https://patents.google.com/patent/US2521084A/en.
-
Ogami S, Yamada M, Kanazawa M, Takeda K, Kimura N, Mizutani H, Kohase H, Fukayama H. The effectiveness of a mouth guard to protect against strong occlusion caused by modified electroconvulsive therapy. Dent Traumatol. 2014;30(5):368-373.
-
Abrams AM. Practical Hints: Boxer’s appliance. The Dental Digest. 1930 March;36(3):200-201.
-
Jacobs WH. Practical Hints: Boxer’s appliance. The Dental Digest. 1930 March;36(3):201.
-
Hagey JW. Practical Hints: Boxer’s appliance. The Dental Digest. 1930 March;36(3):201-202.
-
Watts G, Woolard A, Singer CE. Functional mouth protectors for contact sports. J Am Dent Assoc. 1954;49(1):7-11.
-
Downing JF. Operation mouthgard. J Sch Health. 1964;34:339-42.
-
Beard CC, Clayton JA. Effects of occlusal splint therapy on TMJ dysfunction. J Prosthet Dent. 1980;44(3):324-35.
-
Goharian RK, Neff PA. Effect of occlusal retainers on temporomandibular joint and facial pain. J Prosthet Dent. 1980;44(2): 206-8.
-
Vauthier F, Spirgi M. La gouttière occlusale et son influence sur l’enregistrement frontal du mouvement d’ouverture maximale et de fermeture dans les cas de troubles algo-dysfonctionnels des articulations temporo-mandibulaires [The occlusal bite splint and its effect on the centric relation of the maximal opening and closing movement in cases of temporomandibular joint syndrome]. SSO Schweiz Monatsschr Zahnheilkd. 1977;87(3):189-208.
-
Haywood VB. Overview and status of mouthguard bleaching. J Esthet Dent. 1991;3(5):157-61.
-
de Melo C, Resende JB, Lozada MIT, Mendoza LCL, Ribeiro MTH, Soares PBF, Soares CJ. Effect of surface treatment of ethylene vinyl acetate on the delamination of custom-fitted mouthguards. Dent Traumatol. 2023;39(4):324-332.
-
Firmiano TC, de Oliveira AA, Costa PVM, Cardoso LS, Pereira RD, Veríssimo C. Influence of different ethylene-vinyl acetate brands used for custom-fitted mouthguard fabrication on the stress and strain during an impact. Dent Traumatol. 2022;38(5):431-438.
-
Grewal N, Kumari F, Tiwari U. Comparative evaluation of shock absorption ability of custom-fit mouthguards with new-generation polyolefin self-adapting mouthguards in three different maxillary anterior teeth alignments using Fiber Bragg Grating (FBG) sensors. Dent Traumatol. 2015;31(4):294-301.
Articole din ediţiile anterioare
INTERDISCIPLINARY | Ediţia 1 62 / 2024
Femei celebre în stomatologie – secolul XX
Mihai Burlibaşa, Viorel Ştefan Perieanu, Bogdan Alexandru Dimitriu, Radu Cătălin Costea, Andrei Burlibaşa, Irina Adriana Beuran, Daniela‑Aurelia Pîrvu, Florentina Căminişteanu, Mircea Popescu, Nicoleta Măru
Emanciparea femeilor, atât în Europa, cât şi în SUA, a început cu adevărat în a doua jumătate a secolului al XIX-lea. După încheierea Primului R...
20 februarie 2024
INTERDISCIPLINARY | Ediţia 1 58 / 2023
Femei celebre în stomatologie – secolele XVIII-XIX
Mihai Burlibaşa, Radu Cătălin Costea, Irina Adriana Beuran, Ioana Maria Stoica, Bogdan Alexandru Dumitru, Nicoleta Măru
După cum am arătat deja şi în prima parte a acestui material, emanciparea femeilor, atât în Europa, cât şi în SUA, a început cu adevărat în a doua ...
03 martie 2023
INTERDISCIPLINARY | Ediţia 4 57 / 2022
Femei celebre în stomatologie – secolele XVIII-XIX
Mihai Burlibaşa, Radu Costea, Irina Adriana Beuran, Ioana Maria Stoica, Bogdan Alexandru Dumitru, Nicoleta Măru
După cum foarte bine se cunoaşte, emanciparea femeilor, atât în Europa, cât şi în SUA, a început cu adevărat în a doua jumătate a secolului al XIX-...
28 noiembrie 2022
INTERDISCIPLINARY | Ediţia 1 62 / 2024
Aspecte tehnologice în confecţionarea gutierelor cu utilizare dentară (Partea a II-a)
Ioana Voinescu, Carmen-Georgiana Dorobanţu, Radu Cătălin Costea, Viorel Ştefan Perieanu, Daniela‑Aurelia Pîrvu, Mircea Popescu, Irina Adriana Beuran, Florentina Căminişteanu, Bogdan Alexandru Dimitriu, Mihai Burlibaşa
În acest material, am încercat să evidenţiem importanţa gutierelor dentare, deoarece acestea sunt utilizate în aproape toate specialităţile afer...
20 februarie 2024