Protein-calorie malnutrition is characterized by the low weight of the child compared to the weight he/she should have at the respective age and, also, the height in relation to the age if the nutritional deficit is long-term. The advances in medical biochemistry have their applicability here, and not only in the technology and the new diagnostic methods in the field of clinical laboratory. However, it is undesirable that the dietetics offices in the pediatric departments of city or county hospitals should be abolished, as well as those in the structure of pediatric clinics in university centers. The forms of protein-caloric malnutrition are presented, as well as the biochemical effectors that initiate the physiopathological process corresponding to the degree of malnutrition. The impact of this metabolic syndrome on the child’s growth and development is also discussed.
Aspecte biochimice şi imunobiologice în malnutriţia protein-calorică la copil
Biochemical and immunobiological aspects in pediatric protein-calorie malnutrition
First published: 31 octombrie 2022
Editorial Group: MEDICHUB MEDIA
DOI: 10.26416/Pedi.67.3.2022.7232
Abstract
Rezumat
Malnutriţia protein-calorică se caracterizează prin greutatea mică a copilului faţă de greutatea pe care ar trebui să o aibă la vârsta respectivă şi, de asemenea, ţinând cont de talia în raport cu vârsta, dacă deficitul nutriţional este pe termen lung. Progresele biochimiei medicale îşi au aplicabilitatea şi aici, nu doar privind tehnologia şi metodele noi de diagnostic în domeniul laboratorului clinic. Este totuşi de nedorit ca oficiile de dietetică din secţiile de pediatrie ale spitalelor orăşeneşti sau judeţene să fie desfiinţate, la fel şi cele din structura clinicilor de pediatrie din centrele universitare. Sunt prezentate formele de malnutriţie protein-calorică, precum şi efectorii biochimici care iniţiază procesul fiziopatologic corespunzător gradului de malnutriţie. De asemenea, este adus în discuţie impactul acestui sindrom metabolic asupra creşterii şi dezvoltării copilului.
Deficiency diseases due to nutritional inadequate and incomplete diets constitute public health problems in several developing countries. Among these, protein energy malnutrition (PEM) is the most well-known. It is a disease predominantly of young children living under unsatisfactory socioeconomic conditions. The severe forms bear a high mortality rate if they don’t receive prompt attention. The less severe forms enforce permanent life-threatening disabilities not only during childhood, but also in the adult life. A very large volume of data is available on PEM, but only the very pertinent features are presented here, with emphasis on the public health aspects. No attempt has been made to be exhaustive.
Malnutrition is characterized, in the acute phase, by a low weight according to the child’s age and, later, in the chronic phase, by low weight for the child’s waist. Malnutrition can occur through insufficient food intake, through increased protein losses in certain conditions, by increasing the need for nutrients (during the growth period) or in various chronic diseases, due to the increased catabolism generated by the drugs administered. This condition includes both undernutrition and obesity. Two forms of malnutrition can be described: acute malnutrition and chronic malnutrition. Malnutrition can be associated with a calorie deficit, protein deficit or protein-calorie deficit(1).
Classification of malnutrition
Depending on the weight index, children with malnutrition can be classified into the following categories:
-
Children whose Body Mass Index represents 75-90% of the normal value of body weight.
-
Children whose Body Mass Index represents 60-75% of the normal value of body weight.
-
Children whose Body Mass Index is below 60% of the normal value of body weight.
Depending on the severity of the clinical manifestations, three forms of malnutrition can be described:
-
mild malnutrition
-
moderate malnutrition
-
severe malnutrition.
-
Depending on the height index value, three forms of malnutrition can be described:
-
Grade I malnutrition, the child’s height representing 90-95% of the age-appropriate height.
-
Grade II malnutrition, the child’s height representing 85-90% of the age-appropriate height.
-
Grade III malnutrition, the child’s waist being below 85% of the age-appropriate height.
-
Depending on the value of the nutritional index, three forms of malnutrition can be described:
-
Grade I malnutrition – the child has a weight of 80-90% of the weight corresponding to the ideal waist.
-
Grade II malnutrition – the child has a weight of 70-80% of the weight corresponding to his age and height.
-
Grade III malnutrition – the child has a weight below 70% of the weight corresponding to his age and height(2,3).
Biochemical and immunobiological aspects in a nutshell
Dendritic cells (DCs) produce cytokines and present antigens to T cells, thus coupling innate and adaptive immunity. Children with kwashiorkor had normal numbers of white blood cells (WBCs), however, although the numbers of monocyte-derived DCs were reduced in their peripheral blood. The malnutrition protein impairments were rectified following intervention using a protein-sufficient diet(3). Antigen presentation to the cells of the adaptive immune system may have been reduced in grade II malnutrition, to decreased numbers of monocyte-derived DCs. Furthermore, Nassar and colleagues reported that Fas (CD95/apoptosis antigen 1), a gene that signals to initiate apoptosis, is highly expressed in neutrophils, monocytes and lymphocytes in kwashiorkor children, indicative of impaired regulation of immunity and lymphoid homeostasis(4). The consequence of nutrient deficiency on immune response and host defense has been primarily studied in protein-calorie malnutrition (PCM) and in micronutrient deficiencies. Undernutrition – especially PCM – is clearly linked with an increased susceptibility to infections and with higher morbidity from infectious complications. Still, the appropriate cause of reduced host defense and increased mortality from acute respiratory tract infections observed in the malnourished child is often related to a combination of factors rather than to a single factor(5).
Micronutrient deficiencies should not be neglected. However, each micronutrient deficiency per se can cause important clinical disorders, with serious alterations in the innate/adaptive immune function and host defense. Micronutrients have as well a crucial influence on immune response, both through antioxidant effects and through regulation of cytokine expression. Oligoelements and vitamins have an antioxidant role through participation in enzyme-catalytic reactions. These reactions are indispensable to offset potential oxidative ruination caused by free radical formation. Three antioxidant enzymes – copper, zinc and manganese superoxide dismutases – require oligometals for biologic activity, and micronutrients are crucial regulators of cytokine production. Parenteral nutrient preparations may not bring adequate levels of micronutrients such as vitamin E and selenium, originating antioxidant deficiency, which may lead to lipid peroxidation, a test of oxidative stress(6). Micronutrients, oligoelements and vitamins exert important regulatory effects on adaptive immune cell function. Specific nutrients, such as zinc, support a Th1 cytokine response in which interleukin 2 (IL-2) and interferon (IFN)-g are produced, contrasting with other nutrients, such as vitamin A, which typically support the secretion of Th2 cytokines, including IL-4, IL-5 and IL-10. For this reason, the ful effect of the microenvironment is to direct the immune response toward either a Th1, or a Th2 response(7).
Neonatological features
We cannot neglect the newborn period, because this would mean giving an incomplete picture of our article. Taking into account the particularities of the child’s development by age stage (newborn, infant, early childhood, preschool, school), these also have their nutritional particularities. We do not want to suggest diets and nutritional schemes here, because this was not the primary purpose of our work. It is very important to underline the fact that it is a big mistake that in city hospitals, county hospitals, and even in some university centers in pediatric clinics, dietetic offices and baby feeding facilities are about to be out of use or not in use. Also, every hospital in which there is a clinic or a pediatric department would be desirable to have staff strictly specialized in infant dietetics.
In this debate, effort will be made to make a distinction between the nutrient effects, which are in general applicable to all tissues, from the direct impact in which lymphoid tissues and immune response are influenced either disproportionately or specifically. In the same way, the mechanism of nutrient action may differ according to setting and concentration and the source. The pharmacologic use of nutrients may have immunomodulatory effects which differ from those exerted by smaller amounts that can contribute to achieve physiologic repletion to standard levels. This dissimilarity may explain why supplementation above normal levels may sometimes be connected with an abolishment of innate immune response that could not have been foretell from studies of repletion. The effect of any supplementation is affected as well by conditions in the host. The presence of infections, underlying illness or a given immune deficiency, may also affect the response to nutrient administration(8).
In terms of nutrition, at the beginning of the newborn period, of course, we will focus on the nutritious biochemical elements and compounds that are contained in the mother’s milk. The neonate needs, as well, oligonutrients such as iron, zinc and selenium, as well as an energy diet. Vitamin A is essential for the development of normal immune response and for the development of lung epithelization. Airway infection in the mechanically ventilated very-low-birth-weight infant was associated, due to decreased plasma vitamin A. Human milk normally contents bioavailable micronutrients such as zinc, as well as secretory immunoglobulin and growth factors(9). Some maternal milk may be lacking in zinc despite normal levels in serum and, in those cases, babies may acquire a condition that is phenotypically similar to acrodermatitis enteropathica. Decreased fatty acids levels, such as docosahexaenoic acid (DHA), in mothers have been found to correspond directly with low levels in malnourished infants. DHA is crucial for visual acuity, impacting postnatal brain growth, and also controlling, somehow, the immune response through inhibitory effects on the IL-2 pathway(10).
Conclusions
The problem of protein-calorie malnutrition involves the approach to many aspects: biochemical, immunological, therapeutic, epidemiological, aspects related to pediatrics and social neuropsychiatry. In this article, we tried to summarize the essence of some biochemical and immunobiological peculiarities without going into details of the therapeutic approach. Malnutrition may have an enduring effect all along the critical periods of the early development, having a definitive effect on the fundamental program of child growth and development. Equipping pediatric departments and clinics with an independent dietetic office, with strictly specialized staff for infant dietetics, is an imperative and desirable utility.
Conflict of interests: The authors declare no conflict of interests.
Bibliografie
-
Merck Manual, 18th Edition, All Publishing House, Bucharest, 2014.
-
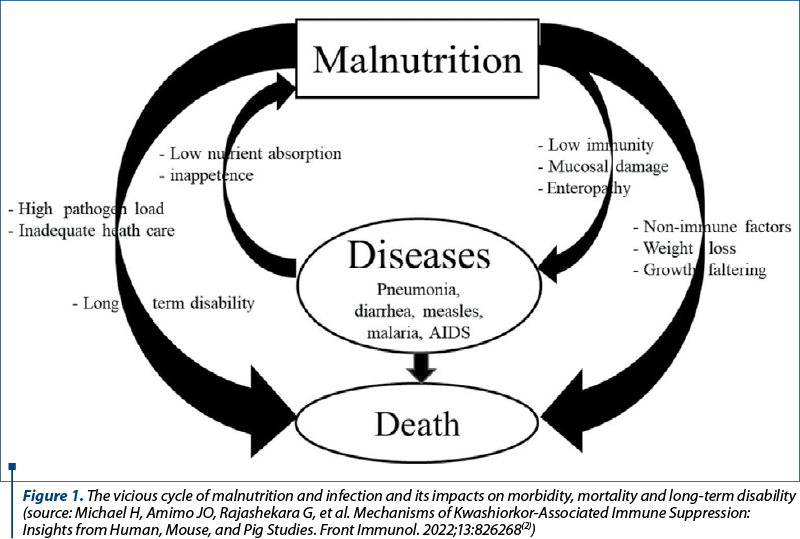
Michael H, Amimo JO, Rajashekara G, Saif LJ, Vlasova AN. Mechanisms of Kwashiorkor-Associated Immune Suppression: Insights from Human, Mouse, and Pig Studies. Front Immunol. 2022;13:826268. doi: 10.3389/fimmu.2022.826268.
-
Hughes SM, Amadi B, Mwiya M, Nkamba H, Tomkins A, Goldblatt D. Dendritic Cell Anergy Results from Endotoxemia in Severe Malnutrition. J Immunol. 2009;183(4):2818–26. doi: 10.4049/jimmunol.0803518.
-
Nassar MF, El-Batrawy SR, Nagy NM. CD95 expression in white blood cells of malnourished infants during hospitalization and catch-up growth. East Mediterr Health J. 2009;15(3):574-583. doi: 10.26719/2009.15.3.574.
-
Lin E, Kotani JG, Lowry SF. Nutritional modulation of immunity and the inflammatory response. Nutrition. 1998;14(6):545-550. doi:10.1016/s0899-9007(98)00046-x.
-
Cunningham-Rundles S. Evaluation of nutrient interaction in immune function. In: Calder PC (ed), Nutrition and immune function, 2002, CABI, pp. 21-39.
-
Beisel, WR 2007, Malnutrition and Immune Response (retrieved January 3, 2007). Available at: http://stinet.dtic.mil/oai/oai?&verb=getRecordPrefix=html&identifier=ADA048384.
-
Cunningham, Rundles, S, McNeeley, D, Ananworanich, JM. Immune response in malnutrition. In: ER Stiehm, HD Ochs, JA Winkelstein (eds). Immunologic Disorder in Infant and Children, 5th ed., 2002.
-
Scrimshaw NS, SanGiovanni JP. Synergism of nutrition, infection, and immunity: an overview. Am J Clin Nutr. 1997;66(2):464S-477S. doi:10.1093/ajcn/66.2.464S.
-
Kelly D, Coutts AG. Early nutrition and the development of immune function in the neonate. Proc Nutr Soc. 2000;59(2):177-185. doi:10.1017/s0029665100000197.
Articole din ediţiile anterioare
Modern treatment methods to reduce mortality and morbidity associated with burns in the pediatric patient
Arsurile pot avea diverse etiologii şi diferite suprafeţe şi grade. În funcţie de gravitate, se pot însoţi de morbiditate şi mortalitate sem...
Tratamentul insuficienţei hepatice acute la copil
Insuficienţa hepatică acută (IHA) este un sindrom caracterizat prin alterarea rapidă a funcţiei hepatice, icter şi coagulopatie severă (o valoare a...
Complexitate patogenică imună: psoriazis și hepatită cronică cu VHB
Hepatitele cronice reprezintă o cauză frecventă de complicaţii cum ar fi ciroza hepatică şi carcinomul hepatocelular, chiar şi în contextul infecţi...
Intervenţii nutriţionale precoce în dislipidemii la vârsta pediatrică și riscul pentru sindrom metabolic
Tulburările metabolismului lipidic reprezintă o patologie relativ frecventă la vârsta pediatrică, existând două etiologii principale: terenul ge...